|
Case Report
Robot-assisted laparoscopic enucleation of prostate with early catheter removal: A case report
1 MD, Urology resident, Division of Urology, Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok, Thailand
2 Urology staff, Division of Urology, Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok, Thailand
3 Research assistant, Division of Urology, Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok, Thailand
4 MD, Associate Professor, Division of Urology, Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok, Thailand
Address correspondence to:
Wisoot Kongcharoensombat
Associate Professor, Division of Urology, Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok,
Thailand
Message to Corresponding Author
Article ID: 100066Z15SS2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Supabphol S, Sirisopana K, Phengsalae Y, Ketsuwan C, Sangkum P, Kongcharoensombat W. Robot-assisted laparoscopic enucleation of prostate with early catheter removal: A case report. J Case Rep Images Urol 2026;11(1):33–39.ABSTRACT
Introduction: Current American Urological Association guidelines on surgical management of benign prostatic hyperplasia (BPH) recommend either laser enucleation techniques or minimally invasive simple prostatectomy for prostates exceeding 150 g. Robot-assisted simple prostatectomy (RASP) has emerged as a safe and effective option to address the anatomical challenges, particularly in centers with established robotic expertise.
Case Report: A 63-year-old Thai male with essential hypertension and chronic kidney disease presented with progressive lower urinary tract symptoms and a rising serum creatinine level. Imaging revealed a markedly enlarged prostate (213 g) with intravesical protrusion and severe bilateral hydronephrosis. Magnetic resonance imaging was further requested to exclude malignancy, as his initial prostate-specific antigen (PSA) level was 13.13 ng/mL. After confirmation of a PI-RADS 2 lesion and discussion of surgical options, patient accepted to undergo RASP. Due to unexpected intraoperative findings of trilobar prostatic enlargement obscuring both ureteric orifices and distorting normal anatomy, our team was forced to switch from conventional simple prostatectomy to enucleation. Each lobe was removed separately as en bloc dissection was impossible. Total operative time was approximately 3 hours with an estimated blood loss of 400 mL. The urethral catheter was retained for four days and removed before discharge. The pathological report confirmed benign prostatic hyperplasia with 168 g of prostatic tissue removed. At one month, the patient was satisfied with lower urinary tract symptom improvement. Uroflowmetry verified a maximal urinary flow rate of 28 mL/s with a post-void residual urine of 10 mL.
Conclusion: Our case confirmed the safety and practicality of robot-assisted laparoscopic enucleation in extremely large prostates with abnormal configuration. This operation serves as another surgical option for patients who desire excellent functional outcomes with minimal urethral stricture and incontinence rates. However, surgeon experience and the learning curve should also be considered as they directly affect postoperative outcomes.
Keywords: Benign prostatic hyperplasia, Prostatic enucleation, Robot-assisted simple prostatectomy, Very large prostate
Introduction
According to recent American Urological Association guidelines on the surgical management of benign prostatic hyperplasia (BPH), only two minimally invasive treatment options are available for very large prostates (larger than 150 g)—laser enucleation techniques and simple prostatectomy [1]. Holmium and Thulium are the two most common laser energy sources applied in endoscopic enucleation of the prostate [2]. Similar to minimally invasive simple prostatectomy (mainly a laparoscopic and robotic approach), Holmium laser enucleation of the prostate (HoLEP) and Thulium laser enucleation of the prostate (ThuLEP) yield excellent International Prostate Symptom Scores (IPSS) and maximum urinary flow rates (Qmax) [3]. With varying considerations, robot-assisted simple prostatectomy (RASP) dominates HoLEP in terms of urethral stricture and urinary incontinence. However, this approach tends to be associated with increased intraoperative blood loss, longer operative times, and longer hospital stays [4].
Robot-assisted radical prostatectomy (RARP) has long been known as the mainstay treatment for localized prostate cancer. This being our experience at Ramathibodi Hospital, mastering RASP requires a shorter learning curve compared to endoscopic enucleation techniques. Over time, our team has concentrated on optimizing the robotic procedure by reducing operative time and length of hospital stay, minimizing blood loss, and lowering the risk of postoperative complications.
To provide a comprehensive overview of RASP, we present a case report describing the key surgical steps and highlighting the advantages of this technique. In this patient, the extremely enlarged prostate completely obscured the prostatic border and ureteric orifices, necessitating prostatic enucleation via a robotic approach rather than a conventional simple prostatectomy. We hope this report may serve as an educational resource for the surgical skill development of urologic surgeons who are interested in adopting the robotic approach for managing very large prostates.
Case Report
A 63-year-old Thai male with underlying diseases of essential hypertension and chronic kidney disease presented at our urology outpatient department with lower urinary tract symptoms (LUTS). He was diagnosed with benign prostatic hyperplasia (BPH) and prescribed a combination of doxazosin and finasteride. During the follow-up period, progressive renal function gradually declined, with serum creatinine rising from 5.0 to 7.0 mg/dL.
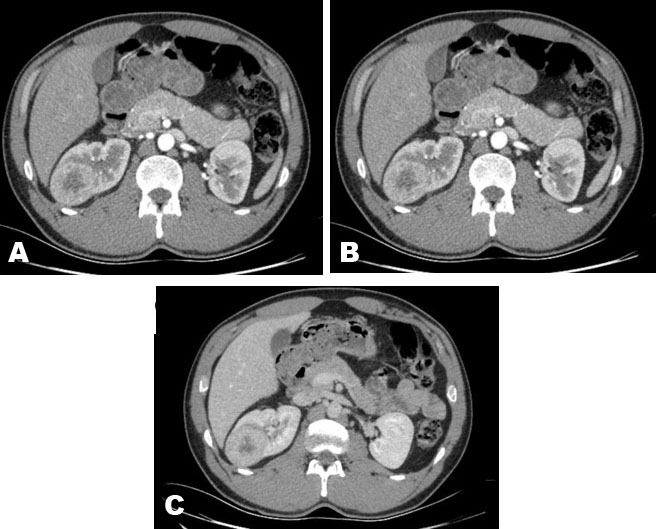
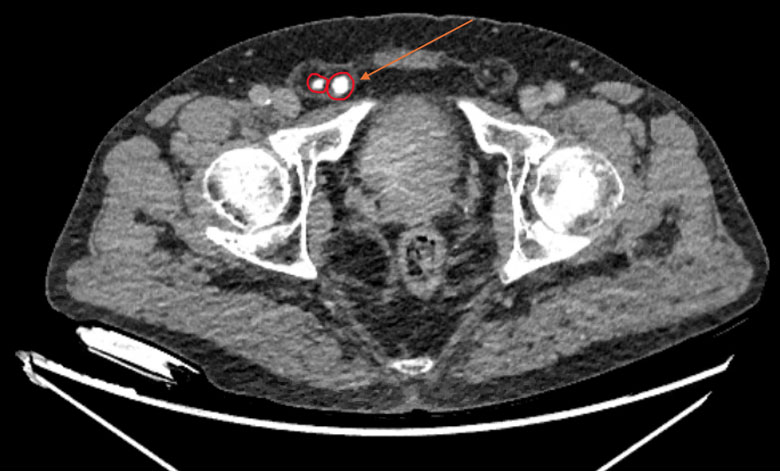
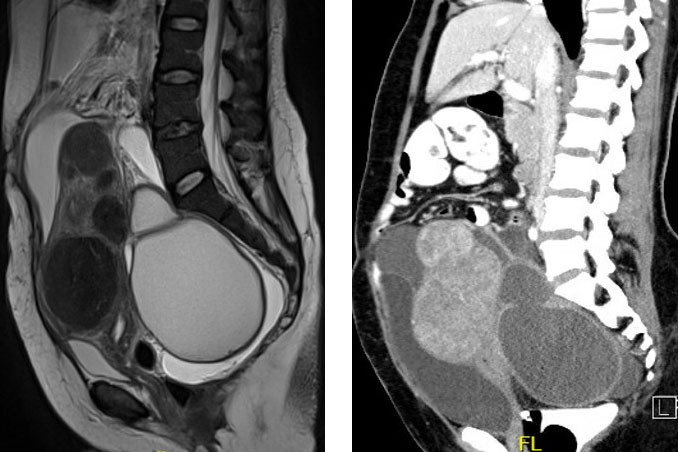
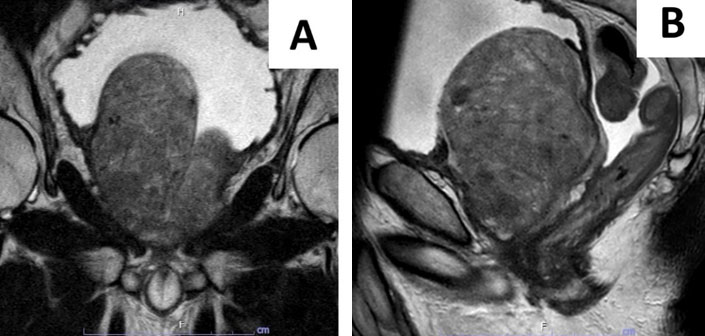
Renal ultrasonography and noncontrast computed tomography (CT) revealed severe bilateral hydronephroses and a markedly enlarged prostate (8.10 × 6.75 × 7.50 cm; calculated volume 213 mL) protruding into the decompensated urinary bladder. The right lobe accounted for most of the prostate volume. Due to postrenal acuteon-chronic kidney disease, a Foley catheter was inserted until renal function recovered. According to nephrologist suggestions, hemodialysis was not required for the patient. Prostate magnetic resonance imaging (MRI) was subsequently performed to exclude malignancy, as the patient’s initial prostate-specific antigen level was 13.13 ng/mL. As expected, the official MRI report included a Prostate Imaging Reporting and Data System (PI-RADS) 2 lesion, consistent with benign pathology, and corroborated the ultrasonography and CT findings. The calculated prostate volume was 187 mL (5.50 × 7.20 × 9.00 cm) with intravesical prostatic protrusion of 9.50 cm (Figure 1). Considering the severity of bladder outlet obstruction and worsening renal function, the surgical indication for BPH was met. After a thorough discussion of the risks and benefits of each treatment option, the patient consented to undergo RASP.
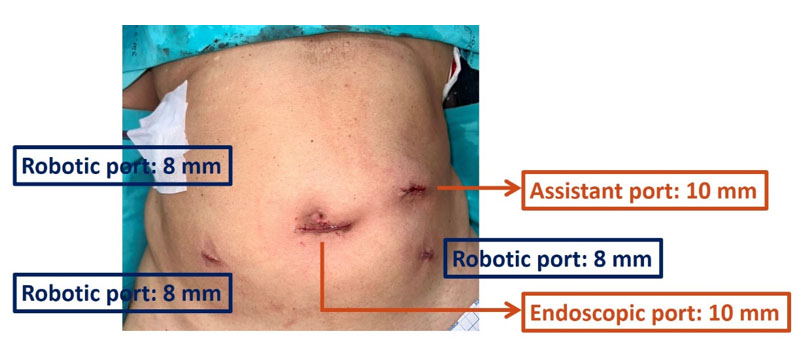
Under general anesthesia, the patient was placed in the Trendelenburg position. Following the standard protocol for RARP, a Foley catheter was inserted, and five robotic ports were placed (Figure 2). The Da Vinci XI robot was docked, and two surgeons operated from the console.
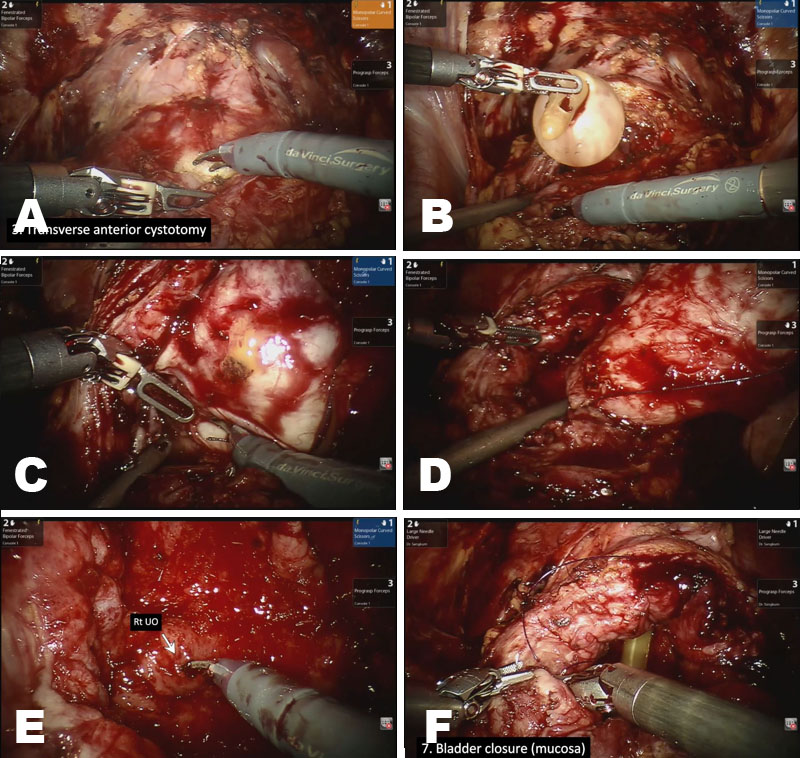
After entering the intraperitoneal space, the umbilical ligament was dissected, allowing the bladder to drop down. A transverse anterior cystotomy was performed approximately 1 cm above the bladder neck (Figure 3A). The Foley catheter was routinely identified and lifted to better visualize the posterior aspect of the prostate (Figure 3B).
Due to extreme trilobar prostatic enlargement, each lobe had to be dissected separately. The enlarged lobes obscured both ureteric orifices and the circumferential border of the prostate, requiring enucleation instead of a conventional simple prostatectomy. First, the right lobe was raised to facilitate dissection, and enucleation was carried out from base to apex (Figure 3C). It was then removed before proceeding to the left lobe enucleation, which was performed in a similar fashion (Figure 3D). Upon completion of enucleation, the ureteric orifices could be clearly identified with no electrocautery injury (Figure 3E). Hemostasis was achieved with coagulation. Notably, vesicourethral anastomosis was not essential, as we enucleated both lobes without transecting the prostatic urethra. The bladder was then reconstructed with a double-layer continuous suture using Stratafix 3-0 and 2-0 sutures (Figure 3F). The specimen was finally retrieved, and a surgical drain was placed through one of the robotic ports.
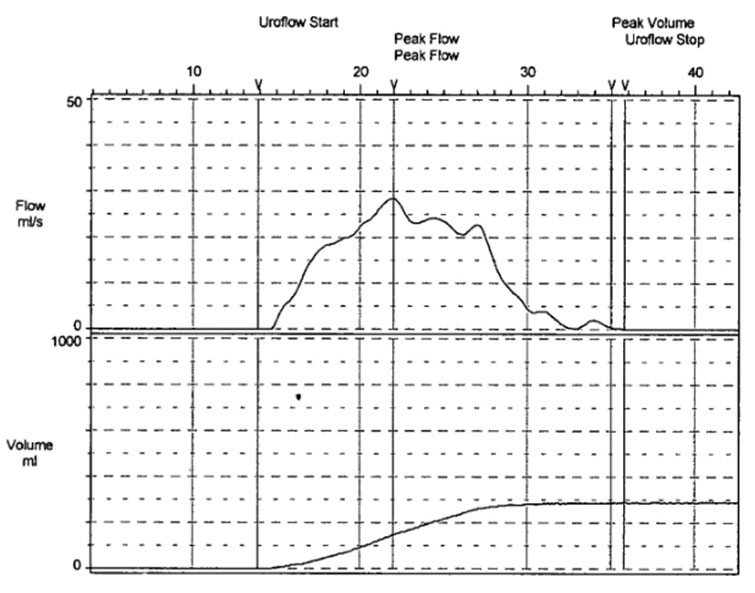
The approximate console time was 3 hours, with an estimated blood loss of 400 mL. The Foley catheter could be successfully removed on postoperative day 4 without the need for a cystogram. The patient experienced no postoperative complications and was discharged after successful voiding. During the follow-up period, his voiding LUTS markedly improved, with high levels of patient satisfaction. A Qmax of 28 mL/s and residual urine of 10 mL were observed in uroflowmetry at one month (Figure 4). No stress or urge urinary incontinence were complained by the patient. The official pathology report confirmed benign prostatic hyperplasia without evidence of malignancy. A total of 168 g of prostatic tissue was resected.
Discussion
Robot-assisted simple prostatectomy has emerged as an effective and satisfactory option for both open simple prostatectomy and laser enucleation techniques for BPH exceeding 150 g [5],[6]. With advantages of lower urethral stricture and incontinence rates, RASP provides postoperative IPSS and Qmax comparable to HoLEP while allowing concomitant vesical calculi removal in cases of large stones [7],[8]. While HoLEP requires at least 50 carefully selected cases to achieve expertise, RASP tends to have a relatively shorter learning curve, especially in academic institutions where RARP is routinely performed [9],[10].
Robot-assisted simple prostatectomy and RASP share similar procedural steps. The key difference is that RARP requires complete removal of the prostate and seminal vesicles, whereas RASP involves removal of only the obstructing adenoma without concern for surgical margins [11]. With experience gained from RARP, both surgical and functional outcomes can be improved in RASP. A recent meta-analysis of the RARP learning curve demonstrated that operative time significantly decreases after approximately 100 cases and stabilizes between 200 and 400 cases. Estimated blood loss also begins to decline after 100–230 cases. However, long-term functional outcomes, including 2-year continence and potency rates, require 200–300 cases to reach a plateau [12]. At our center, approximately 200–220 RARP cases are performed annually, providing substantial experience and confidence in transferring robotic surgical skills to RASP.
Our case confirmed the safety and practicality of robot-assisted laparoscopic prostatic enucleation in a patient with a markedly enlarged prostate (213 g) obscuring both ureteric orifices and the surrounding prostatic border. Converting from the conventional simple prostatectomy to an enucleation-based approach allowed better visualization of prostate anatomy [13],[14]. If conventional simple prostatectomy had proceeded, surgeons might have dissected through the prostatic adenoma and resulted in unexpected bleeding. In addition, enucleation without transecting the prostatic urethra avoids vesicourethral anastomosis, which impedes early Foley catheter removal. With our surgical proficiency in the robotic approach, we were able to minimize blood loss and reduce operative time to values approaching those reported for laser enucleation techniques. The patient experienced an uncomplicated recovery with early catheter removal, short hospitalization, and excellent postoperative functional outcomes.
Cost and accessibility remain significant obstacles for robotic platforms, as they are not universally available and are associated with substantial capital and maintenance expenses [15]. In contrast, beyond the advantages of estimated blood loss and length of hospital stay, HoLEP equipment is more widely available and is not prohibitively expensive [16]. Additionally, HoLEP is supported by more than two decades of follow-up data, including randomized controlled trials demonstrating excellent outcomes and low retreatment rates beyond 10 years [17]. By comparison, long-term data for RASP are still relatively limited, although early and mid-term studies consistently report excellent symptomatic and functional results [18]. Continued accumulation of evidence from multi-institutional registries and randomized trials will be critical for further defining its role.
Finally, the selection of RASP or laser enucleation techniques takes into account several factors, including surgeon expertise, available surgical instruments, patient comorbidities, and patient preference. No single technique is suitable for all patients. For individuals who are highly concerned about urethral stricture and incontinence, or who have concomitant large vesical calculi—particularly in institutions with established robotic platforms—RASP offers a highly effective, adaptable, and safe surgical solution. However, in places where robotic access is limited, laser enucleation remains an excellent alternative with proven long-term outcomes.
Conclusion
Robot-assisted simple prostatectomy is widely recognized as another minimally invasive therapeutic option for BPH in which the prostatic volume exceeds 150 g. It provides excellent postoperative IPSS and Qmax with minimal rates of urethral stricture and incontinence. However, selecting the operation depends on surgeon experience and the patient’s preoperative factors and preference. We hope this case presentation can serve as a practical guide for urologic surgeons to master their operative skills and achieve better postoperative outcomes.
REFERENCES
1.
Sandhu JS, Bixler BR, Dahm P, Goueli R, Kirkby E, Stoffel JT, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia (BPH): AUA guideline amendment 2023. J Urol 2024;211(1):11–19. [CrossRef]
[Pubmed]

2.
Hartung FO, Kowalewski KF, von Hardenberg J, Worst TS, Kriegmair MC, Nuhn P, et al. Holmium versus thulium laser enucleation of the prostate: A systematic review and meta-analysis of randomized controlled trials. Eur Urol Focus 2022;8(2):545–54. [CrossRef]
[Pubmed]
3.
Kim BH, Byun HJ. Robotic-assisted simple prostatectomy versus holmium laser enucleation of the prostate for large benign prostatic hyperplasia: A single-center preliminary study in Korea. Prostate Int 2022;10(3):123–8. [CrossRef]
[Pubmed]
4.
Kim HS, Shin YS. Robotic-assisted simple prostatectomy ver. holmium laser enucleation of the prostate for patients with huge benign prostatic hyperplasia. World J Mens Health 2023;41(4):753–8. [CrossRef]
[Pubmed]
5.
Xia Z, Li J, Yang X, Jing H, Niu C, Li X, et al. Robotic-assisted ver. open simple prostatectomy for large prostates: A meta-analysis. Front Surg 2021;8:695318. [CrossRef]
[Pubmed]
6.
John H, Wagner C, Padevit C, Witt JH. From open simple to robotic-assisted simple prostatectomy (RASP) for large benign prostate hyperplasia: The time has come. World J Urol 2021;39(7):2329–36. [CrossRef]
[Pubmed]
7.
Van der Jeugt J, Umari P, Mottaran A, Ribeiro L, Lambert E, Vollemaere J, et al. Holmium laser enucleation of the prostate ver. robot-assisted simple prostatectomy for lower urinary tract symptoms in patients with extremely large prostates ≥200 cc: A comparative analysis. J Endourol 2023;37(8):895– 902. [CrossRef]
[Pubmed]
8.
Kordan Y, Canda AE, Köseoğlu E, Balbay D, Laguna MP, de la Rosette J. Robotic-assisted simple prostatectomy: A systematic review. J Clin Med 2020;9(6):1798. [CrossRef]
[Pubmed]
9.
Shelton TM, Drake C, Vasquez R, Rivera M. Comparison of contemporary surgical outcomes between holmium laser enucleation of the prostate and robotic-assisted simple prostatectomy. Curr Urol Rep 2023;24(5):221–9. [CrossRef]
[Pubmed]
10.
Wenk MJ, Hartung FO, Egen L, Netsch C, Kosiba M, Grüne B, et al. The long-term learning curve of holmium laser enucleation of the prostate (HoLEP) in the en bloc technique: A single-surgeon series of 500 consecutive cases. World J Urol 2024;42(1):436. [CrossRef]
[Pubmed]
11.
Huynh LM, Ahlering TE. Robot-assisted radical prostatectomy: A step-by-step guide. J Endourol 2018;32(Suppl 1):S28–32. [CrossRef]
[Pubmed]
12.
Tokas T, Mavridis C, Bouchalakis A, Nakou CM, Mamoulakis C. Learning curves in robotic urological oncological surgery: Has anything changed during the last five years? Cancers (Basel) 2025;17(8):1334. [CrossRef]
[Pubmed]
13.
Franco A, Ditonno F, Manfredi C, Licari LC, Bologna E, Cherullo EE, et al. Robot-assisted single-port transvesical enucleation of the prostate: Step-by-step technique and early single-centre experience. BJU Int 2024;133(6):778–82. [CrossRef]
[Pubmed]
14.
Cho JM, Moon KT, Yoo TK. Robotic simple prostatectomy: Why and how? Int Neurourol J 2020;24(1):12–20. [CrossRef]
[Pubmed]
15.
Bejrananda T, Khaing W, Veettil SK, Thongseiratch T, Chaiyakunapruk N. Economic evaluation of robotic-assisted radical prostatectomy: A systematic review and meta-analysis. Eur Urol Open Sci 2025;72:17–28. [CrossRef]
[Pubmed]
16.
Wymer KM, Narang G, Slade A, Sharma V, Thao V, Borah BJ, et al. Evaluation of the cost-effectiveness of surgical treatment options for benign prostatic hyperplasia. Urology 2023;171:96–102. [CrossRef]
[Pubmed]
17.
Fallara G, Capogrosso P, Schifano N, Costa A, Candela L, Cazzaniga W, et al. Ten-year follow-up results after holmium laser enucleation of the prostate. Eur Urol Focus 2021;7(3):612–7. [CrossRef]
[Pubmed]
18.
Morozov A, Bogatova S, Bezrukov E, Singla N, Teoh JY, Spivak L, et al. A systematic review of robot-assisted simple prostatectomy outcomes by prostate volume. World J Urol 2024;42(1):565. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to thank the research assistance unit of the Department of Surgery, Ramathibodi Hospital, Faculty of Medicine, Mahidol University, Bangkok, Thailand for their valuable support and guidance throughout the ethical approval process.
Author ContributionsSuangson Supabphol - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kun Sirisopana - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yada Phengsalae - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Chinnakhet Ketsuwan - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Premsant Sangkum - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Wisoot Kongcharoensombat - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Suangson Supabphol et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.