|
Case Report
Uretero-inguinal herniation: A surprise content in the inguinal canal
1 Core Surgical Trainee, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
2 Consultant Urology Surgeon, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
3 Consultant Transplant and HPB Surgeon, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
Address correspondence to:
Jake Vaughan
Core Surgical Trainee, Oxford University Hospitals NHS Foundation Trust, Oxford,
United Kingdom
Message to Corresponding Author
Article ID: 100064Z15JV2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Vaughan J, Gietzmann W, Udupa V. Uretero-inguinal herniation: A surprise content in the inguinal canal. J Case Rep Images Urol 2026;11(1):26–29.ABSTRACT
Introduction: Inguinal hernias account for over 75% of abdominal wall hernias, with a global prevalence of 7.7%. While bladder involvement occurs in 1–4% of cases, ureteral herniation is rare. Due to non-specific or absent clinical symptoms, uretero-inguinal hernias may remain undiagnosed pre-operatively, posing significant risk of iatrogenic ureteric injury during surgical repair.
Case Report: A 68-year-old man presented with recurrent urinary tract infections and lower urinary tract symptoms, with a background of previous transurethral resection of prostate. Renal ultrasound demonstrated a right sided hydronephrosis, and computed tomography (CT) urogram identified a right inguinal hernia containing a loop of the right ureter, resulting in in ureteric obstruction and hydronephrosis. Antegrade and retrograde stenting were not feasible due to degree of angulation and excess ureteric length. He underwent an open mesh repair of hernia was performed where a redundant loop of ureter was identified within the inguinal canal. The ureter was carefully reduced without resection, and mesh repair was completed. Post-operative imaging confirmed complete resolution of hydronephrosis.
Conclusion: Uretero-inguinal hernia is a rare but clinically significant cause of hydronephrosis and urinary symptoms. Computed tomography urogram is essential for accurate diagnosis and pre-operative planning, reducing risk of ureteric injury. Early recognition and multidisciplinary management are key to achieve a safe surgical outcome.
Keywords: Hydronephrosis, Inguinal hernia, Ureteric obstruction, Uretero-inguinal hernia
Introduction
Inguinal hernia are an extremely common pathology and account for more than 75% abdominal wall hernias and an estimated global prevalence of 7.7% [1]. The presence of bladder within an inguinal hernia is estimated between 1% and 4%; however, ureteral presence in the hernia is rare [2]. Due to a lack of or non-specific clinical symptoms, uretero-inguinal hernias often go unidentified which causes significant risk of iatrogenic injury during repair, including ureteral ligation [3].
Case Report
A 68-year-old male presented with recurrent urinary tract infections (UTIs) and lower urinary tract symptoms (LUTS), with a past history of transurethral resection of the prostate in 2017. He reported no visible groin swelling or pain.
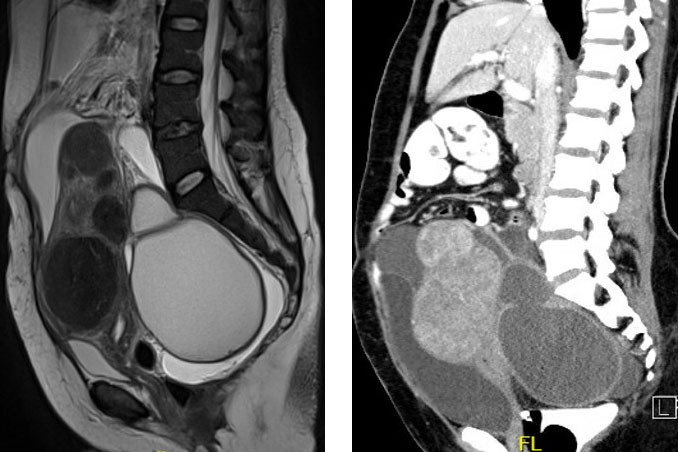
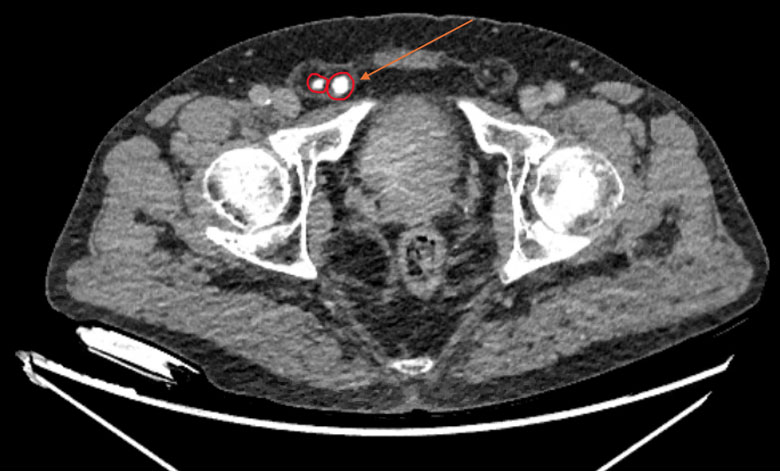
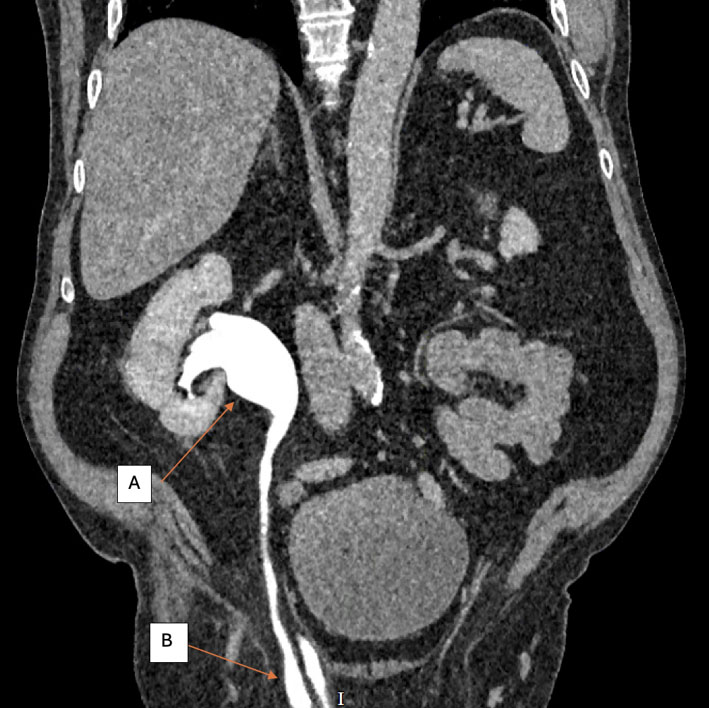
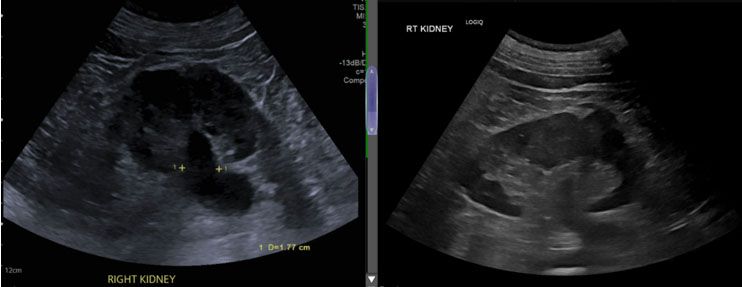
Ultrasound of the kidneys revealed right-sided hydronephrosis, prompting further evaluation with a CT urogram. This demonstrated a right-sided inguinal hernia containing the right ureter (Figure 1), which was compressed within the hernia, resulting in hydronephrosis (Figure 2); however, there was no bladder outflow tract obstruction.
Surgical repair was recommended to prevent progression of hydronephrosis and subsequent renal dysfunction, as well as to reduce the risk of ongoing obstruction and potential ureteric strangulation within the hernia.
Ultrasound demonstrated right pelvicalyceal dilatation, as renal function was not impaired, a nephrostomy was not performed, and antegrade stent insertion was deemed very unlikely to succeed due to a 180-degree angulation of the ureter.
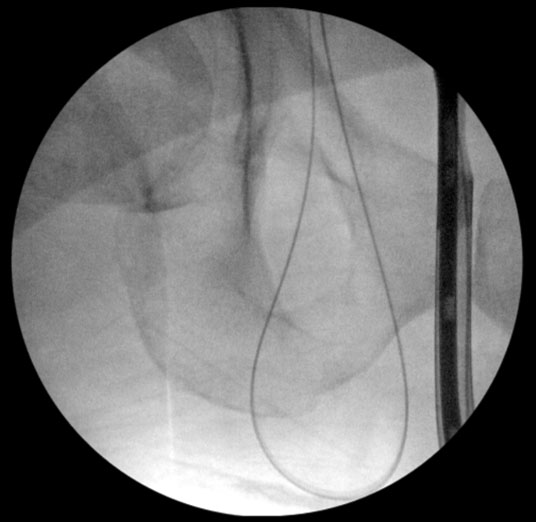
He was subsequently reviewed in the general surgical clinic, on examination he had a right sided inguinal hernia with a small scrotal component, he was listed for open mesh repair of the inguinal hernia, with the recommendation for a pre-operative ureteric stent. Given the challenging ureteric course, a retrograde stent was attempted. Wire cannulation of the right ureter was successful (Figure 3); however, the effective ureteric length measured approximately 50 cm from the bladder, rendering stent placement technically impossible.
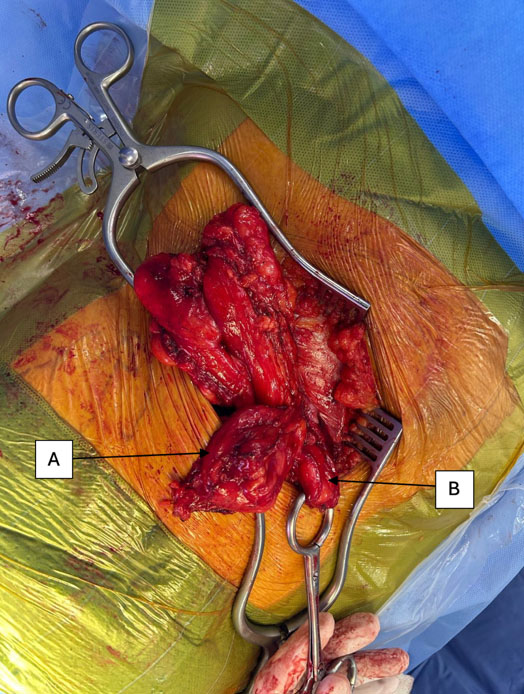
The decision was therefore made to proceed with open mesh repair of the inguinal hernia, with clear acknowledgement of the risk of ureteric injury. An open repair was recommended due to limited reported cases of laparoscopic repair for uretero-inguinal hernia in the literature. Intra-operatively, a large loop of ureter was identified within the inguinal canal, along with retroperitoneal fat, though no discrete hernia sac was present (Figure 4). The redundant ureter was reduced without excision. Prophylactic excision of excess ureter/reimplantation was considered but not performed due to potential for significant complication (urine leak, anastomotic stricture). The distal ureter was identified and reduced to the level of the deep inguinal ring, and the proximal segment was returned to the retroperitoneum, ensuring a tension-free course and preventing twisting or kinking. The hernia was repaired using a Progrip mesh and completed without complication.
To facilitate ureteric identification and minimize the risk of iatrogenic injury, the procedure could be undertaken jointly by urology and general surgery, with pre-operative ureteric catheterization to aid intra-operative localization. However, a dual-specialty approach was not feasible at our center.
Post procedure, an ultrasound showed complete resolution of hydronephrosis (Figure 5).
Discussion
Ureteral herniation is a rare phenomenon and has been described in the literature in several locations; inguinal, femoral, sciatic, obturator and thoracic.
Although ureteral-inguinal hernia is rare it is clinically important. Most cases occur in elderly men, and the right side is more frequently involved. Risk factors include male sex, increased age and history of renal transplant [4].
Previously reported cases have presented with enlarging inguinoscrotal lump, groin pain, lower urinary tract symptoms, hematuria and acute urinary obstruction, or double phase micturition [5].
- Paraperitoneal type (≈80%): the ureter is drawn into the sac alongside peritoneum. Thought to be due to adherence of ureter to hernial sac posteriorly.
- Extraperitoneal type: the ureter herniates alone, without peritoneum. Thought to be congenital. These hernias are a result of an embryological anomaly where the ureteric bud separates from the Wolffian duct late in development as it descents to form the epididymis and testis or adhesions to genito-inguinal ligament [7].
Our patient presented atypically, with recurrent UTIs and a groin lump only detectable on examination. Hydronephrosis was secondary to impaired drainage from ureteric kinking within the hernia. Elective repair of inguinoscrotal hernia is recommended to prevent obstruction, renal dysfunction and potential ureteric strangulation [8]. Recognition on CT urogram was critical to avoid repeated endoscopic interventions or inadvertent intra-operative injury.
Conclusion
Uretero-inguinal hernia is a rare but important cause of urinary tract symptoms and hydronephrosis, and should be considered in patients with unexplained hydronephrosis or abnormal groin anatomy. Computed tomography urogram is the most useful modality for diagnosis, enabling pre-operative recognition that guides appropriate referral for hernia repair and helps preserve the ureter. In this case, accurate imaging prevented repeated unsuccessful interventions and facilitated safe surgical planning. Greater clinical awareness of this entity is essential to avoid ureteric injury and ensure optimal patient management.
REFERENCES
1.
Abebe MS, Tareke AA, Alem A, Debebe W, Beyene A. Worldwide magnitude of inguinal hernia: Systematic review and meta-analysis of population-based studies. SAGE Open Med 2022;10:20503121221139150. [CrossRef]
[Pubmed]

2.
Pasquale MD, Shabahang M, Evans SR. Obstructive uropathy secondary to massive inguinoscrotal bladder herniation. J Urol 1993;150(6):1906–8. [CrossRef]
[Pubmed]
3.
Hwang CM, Miller FH, Dalton DP, Hartz WH. Accidental ureteral ligation during an inguinal hernia repair of patient with crossed fused renal ectopia. Clin Imaging 2002;26(5):306–8. [CrossRef]
[Pubmed]
4.
Morrison Z, Nirujogi VL. Ureteroinguinal hernia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026.
[Pubmed]
5.
McKay JP, Organ M, Bagnell S, Gallant C, French C. Inguinoscrotal hernias involving urologic organs: A case series. Can Urol Assoc J 2014;8(5–6):E429–32. [CrossRef]
[Pubmed]
6.
Roach SC, Moulding F, Hanbidge A. Inguinal herniation of the ureter. AJR Am J Roentgenol 2005;185(1):283. [CrossRef]
[Pubmed]
7.
Lu A, Burstein J. Paraperitoneal inguinal hernia of ureter. J Radiol Case Rep 2012;6(8):22–6. [CrossRef]
[Pubmed]
8.
Gallegos NC, Dawson J, Jarvis M, Hobsley M. Risk of strangulation in groin hernias. Br J Surg 1991;78(10):1171–3. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Artificial intelligence (AI) use in the article:
AI is used for formatting. No generative AI is used.
Jake Vaughan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
W Gietzmann - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
V Udupa - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 J Vaughan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.