|
Case Report
Intraperitoneal bladder perforation presenting as small bowel obstruction in a patient with a chronic indwelling catheter
1 Department of Urology, Madigan Army Medical Center, Tacoma, WA, USA
2 Uniformed Services University of Health Sciences, Bethesda, MD, USA
Address correspondence to:
Timothy W Wright
Honolulu, HI,
USA
Message to Corresponding Author
Article ID: 100061Z15TW2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Wright TW, Li M, Salter CA. Intraperitoneal bladder perforation presenting as small bowel obstruction in a patient with a chronic indwelling catheter. J Case Rep Images Urol 2026;11(1):11–14.ABSTRACT
Introduction: This case describes an unusual presentation of a bladder perforation following a routine catheter exchange in an elderly patient with a chronic indwelling foley catheter.
Case Report: The patient presented with nausea, vomiting, and abdominal distension 10 days after routine exchange of his indwelling foley catheter. He was subsequently diagnosed with a small bowel obstruction. On imaging, he had a transition point at what was potentially the tip of the foley catheter protruding outside of his bladder versus the foley in a small bladder diverticulum. He ultimately required multimodal imaging, cystoscopy, and exploratory laparoscopy for diagnosis. Intraoperative findings ultimately demonstrated an intraperitoneal bladder perforation with the small bowel wrapped around the protruding foley catheter.
Conclusion: Intraperitoneal bladder perforation can present without classic precipitating factors and should be on the differential diagnosis for a patient with bowel obstruction and a recent urinary catheter placement.
Keywords: Bladder perforation, Case report, Chronic indwelling catheter, Small bowel obstruction
Introduction
The Foley catheter is one of the most common pieces of medical equipment urologists utilize. Despite its range of applications, urinary tract infections (UTI), urethral erosion, and discomfort are common complications of use. Rarely, more serious complications can occur, such as malposition of the catheter during placement, which can lead to creation of a false passage in the urethra, premature inflation of the balloon within the prostate fossa, or, in extremely rare cases, bladder perforation. Reports of this complication are scarce in the literature, and we present a unique case in which the patient presented in delayed fashion after a routine catheter exchange with a clinical presentation that was atypical for his ultimate diagnosis of intraperitoneal bladder rupture.
The first recorded case of bladder perforation associated with indwelling catheter was in 1973 [1]. Additional reports have been published since that time, with presenting symptoms most commonly being abdominal pain, distension, peritoneal signs [2],[3],[4],[5],[6], or gross hematuria [5],[7]. The majority of these injuries were identified acutely after catheter placement [4],[5],[6],[8]. In this report, we present a case of intraperitoneal bladder perforation identified in a patient with a small bowel obstruction developing nearly two weeks after a routine catheter exchange.
In the literature, three patients who presented with small bowel obstruction were identified to have underlying bladder perforations [9],[10], though in these cases a length of catheter was clearly visible beyond the bladder wall on imaging [9], and in one case the catheter balloon had been inflated within the lumen of the terminal ileum [10], making for a clear diagnosis. In the following case report, the patient not only lacked the typical peritoneal signs that accompany an intraperitoneal bladder perforation, but their initial imaging was also inconclusive regarding whether the catheter had perforated the bladder, and computed tomography (CT) cystogram was required to confirm the diagnosis.
Case Report
The patient was a frail 86-year-old male with a history of chronic urinary retention due to enlarged prostate managed for several years with a chronic indwelling urethral Foley catheter. The patient presented to the emergency room 10 days following his most recent catheter change, with one day of abdominal distension, nausea, and emesis without notable abdominal pain. Per chart documentation and according to the patient, the catheter change was unremarkable with no difficulty with placement or abnormal urine return. The patient had prior surgical history of open right inguinal hernia repair two years prior, known easily reducible left inguinal, and an umbilical hernia.
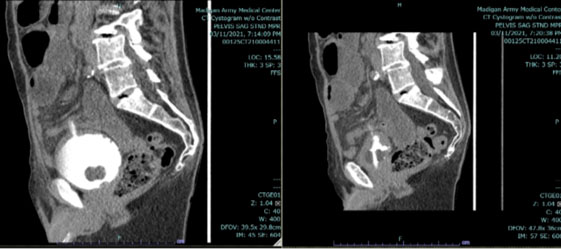
Initial evaluation revealed normal vital signs, normal white blood cell count, basic metabolic panel, and a lactate of 2.9, as well as urinalysis consistent with indwelling Foley. Physical examination revealed a cachectic elderly male with soft, non-tender abdomen, and clear yellow urine was observed in the catheter tube. Computed tomography abdomen and pelvis with intravenous (IV) contrast was obtained and revealed evidence of small bowel obstruction with two possible transition points in the left inguinal region and near the tip of the Foley catheter, which appeared to be either protruding through the dome of the bladder or seated within a small bladder diverticulum (Figure 1). Since the relationship of the catheter to the bladder wall could not be clearly defined, a CT cystogram was also obtained, which demonstrated contrast within a tract extending through the dome of the bladder without free fluid elsewhere in the abdomen or pelvis, suggestive of a contained perforation (Figure 2).
Given the suspicion for an intraperitoneal perforation as the causative agent for the small bowel obstruction, the decision was made to proceed to the operating room (OR) with general surgery and urology for exploratory laparoscopy. Cystoscopy was first performed, revealing a trabeculated bladder with a small defect in the bladder dome, consistent with a diverticulum or a small, contained perforation. The abdomen was then entered laparoscopically, and small bowel was visualized adhered to the distended bladder. Lysis of adhesions was performed and revealed a perforation in the bladder wall with active extravasation of the irrigation fluid from the prior cystoscopy. The defect was repaired laparoscopically with absorbable suture, and the patient had return of bowel function on postoperative day two. Four weeks following the repair, cystogram was performed in clinic prior to catheter change and revealed no evidence of urine leak (Figure 3). The patient continues to be managed with indwelling catheter and has had no subsequent complications.


Discussion
This patient provided an interesting diagnostic challenge, as both his symptoms and his initial imaging were unusual for the diagnosis of intraperitoneal bladder perforation. Spontaneous bladder perforation is very rare, and the cause is not completely understood, though it has been hypothesized to be associated with the negative pressure created by the catheter pulling on the dome of the bladder, which is usually the thinnest point in the detrusor muscle [3],[9]. Additional contributing risk factors that may further weaken the bladder include infection, inflammation, chronic outlet obstruction, distended bladder, long-term catheter use, tumor, and older age, with peak incidence occurring in patients in their 70s or 80s [6]. While not studied in bladder rupture specifically, there is a known increased risk of urinary fistula formation in patients with poor nutrition status [11]. This patient had many of these risk factors present concurrently, with his advanced age, cachexia, prolonged catheter use, and long history of bladder outlet obstruction and chronic urinary retention.
Although the patient was at an increased risk for his injury, the exact mechanism by which his bladder ruptured remains unclear, as the patient’s catheter placement was reportedly unremarkable, the catheter continued to function appropriately after placement, and the patient did not present with the typical symptoms of an intraperitoneal bladder rupture.
It could be theorized that, given the patient’s frail status and relative immobility, the tip of the catheter was in prolonged contact with a weak point in the bladder wall and eroded through the detrusor muscle but remained within the perforation, tamponading the leakage of urine and preventing the development of the peritonitis and acute illness that is classic to an intraperitoneal rupture. If this were the case, in theory the injury could have been self-limited until the presence of the catheter tip in the peritoneum eventually caused a foreign-body reaction leading to the small bowel obstruction.
Conclusion
Although exceedingly rare, spontaneous bladder perforation is a potential complication of indwelling catheter use, and, as this case demonstrates, does not always present with peritonitis and critical illness, especially in patients with risk factors that increase their risk for perforation. To our knowledge, this is the fourth documented case of small bowel obstruction secondary to indwelling urethral foley catheter, and the first case with such an insidious onset of symptoms. In this unique case, the diagnosis was only conclusively revealed by the empty phase of the cystogram demonstrating contrast outside of the bladder, highlighting the importance of a thorough workup with optimal imaging studies, especially for an elderly patient at increased risk for this unusual diagnosis.
REFERENCES
1.
Almgren B, Bergqvist D, Hedelin H. Intraperitoneal bladder perforation caused by indwelling Foley catheter. Scand J Urol Nephrol 1977;11(3):297–9. [CrossRef]
[Pubmed]

2.
Merguerian PA, Erturk E, Hulbert WC Jr, Davis RS, May A, Cockett AT. Peritonitis and abdominal free air due to intraperitoneal bladder perforation associated with indwelling urethral catheter drainage. J Urol 1985;134(4):747–50. [CrossRef]
[Pubmed]
3.
Okuda H, Tei N, Shimizu K, Imazu T, Yoshimura K, Kiyohara H. Experitoneal bladder perforation due to in-dwelling urethral catheter successfully treated by urethral drainage: A case report. [Article in Japanese]. Hinyokika Kiyo 2008;54(7):501–4.
[Pubmed]
4.
Zhan C, Maria PP, Dym RJ. Intraperitoneal urinary bladder perforation with pneumoperitoneum in association with indwelling foley catheter diagnosed in emergency department. J Emerg Med 2017;53(5):e93–6. [CrossRef]
[Pubmed]
5.
Poola S, Mohan A. A Foley fallacy: A case of bladder rupture after “routine” Foley catheter placement. Case Rep Urol 2018;2018:7978126. [CrossRef]
[Pubmed]
6.
Terra C, Cruz M, Portilha MA, Semedo L. Small bowel obstruction secondary to a Foley catheter perforating the bladder: A case report. BMJ Case Rep 2021;14(4):e241076. [CrossRef]
[Pubmed]
7.
Ogawa S, Date T, Muraki O. Intraperitoneal urinary bladder perforation observed in a patient with an indwelling urethral catheter. Case Rep Urol 2013;2013:765704. [CrossRef]
[Pubmed]
8.
Sullivan LP, Davidson PG, Kloss DA, D’Anna JA Jr. Small-bowel obstruction caused by a long-term indwelling urinary catheter. Surgery 1990;107(2):228–30.
[Pubmed]
9.
Magee GD, Marshall SG, Wilson BG, Spence RA. Perforation of the urinary bladder due to prolonged use of an indwelling catheter. Ulster Med J 1991;60(2):237–9.
[Pubmed]
10.
Sayedin H, Datta S, Keoghane S. Laparoscopic repair of catheter-induced intra-peritoneal bladder perforation. Cureus 2021;13(12):e20096. [CrossRef]
[Pubmed]
11.
Ahmad S, Nishtar A, Hafeez GA, Khan Z. Management of vesico-vaginal fistulas in women. Int J Gynaecol Obstet 2005;88(1):71–5. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Timothy W Wright - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mengchuan Li - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Carolyn A Salter - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Disclaimer
The views expressed are those of the author(s) and do not reflect the official policy of the Department of the Army, the Department of Defense, or the U.S. Government. The investigators have adhered to the policies for protection of human subjects as prescribed in 45 CFR 46.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Timothy W Wright et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.