 |
Case Report
Complete left ureter replacement using appendiceal interposition
1 Urology Department, Rouen University Hospital, Rouen, France
2 Radiology Department, Rouen University Hospital, Rouen, France
Address correspondence to:
Marion Ghenassia
MD, Urology Department, Rouen University Hospital, Rouen,
France
Message to Corresponding Author
Article ID: 100037Z15MG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ghenassia M, Bedel JP, Surlemont L, Pfister C, Vangheluwe L. Complete left ureter replacement using appendiceal interposition. J Case Rep Images Urol 2023;8(2):18–21.ABSTRACT
Introduction: Emergency ureteral replacement for large defect, especially in dilapidated abdominal cancer surgery remains an important surgical challenge. Several methods have been described. Here we aimed to present the complete left ureter replacement using appendix interposition, after a large resection of a rectosigmoid mass invading both ureter and iliac artery.
Case Report: A 64-year-old male patient diagnosed of a rectosigmoid hinge lesion invading the ureter and iliac artery. He underwent a large tumor resection. The left ureter was cut during the surgery below the renal pelvis with a loss of substance of more than 12 cm. The procedure involved replacement of the ureter by appendix interposition, with wire drainage by transvesicoparietal catheter and a bladder catheter. Neither ureterohydronephrosis nor urinary fistula was observed at the 2-month follow-up computed tomography.
Conclusion: In our experience, appendiceal interposition in extensive left ureteral defect is a feasible and safe surgical option.
Keywords: Appendiceal interposition, Large ureteral defect, Ureteral reconstruction
Introduction
The replacement of large ureteral defect remains an important challenge in urological surgery. The optimal ureteral substitute should have peristalsis to optimize drainage, a good vascularization, minimize absorption stricture and stone formation, and ideally not permit urine reflux. Many techniques have been proposed for ureteral substitution; among these, for the large and proximal defect, only intestinal ureteral replacement such as ileal ureter, Yang-Monti, appendiceal interposition, and colon substitution have been reported [1],[2],[3].
The use of appendix for ureteral defect was first reported by Melnikoff in 1912 [4], its small caliber, intrinsic peristalsis, exclusive vascularization and little tendency to dilation over time make it a suitable ureteral substitute. The earliest studies about appendiceal interposition have been published in pediatric population [5],[6],[7], and showed good long terms results. There are few retrospective studies in adult population with long-term results [8],[9], but most are for right ureter.
The authors report a case of complete left ureter replacement with appendiceal interposition in antiperistaltic position.
Case Report
The patient was a 64-year-old male with a rectosigmoid adenocarcinoma discovered following abdominal pain. Abdominopelvic computed tomography (CT) revealed probable invasion of the small bowel, bladder, left iliac artery, and left ureter. No distant lesions were noted and cystoscopy was normal. Double J stent was operatively implanted to locate the ureters during surgery. The patient was initially treated with chemotherapy (6 courses of Folfox).
He underwent a large resection of the digestive tumor, which included resection of the rectosigmoid hinge mass, resection of the external iliac artery (repaired with an ilio-iliac bypass), and resection of the left ureter at renal pelvis level.
We opted for a complete left ureteral reconstruction using appendicular transposition.
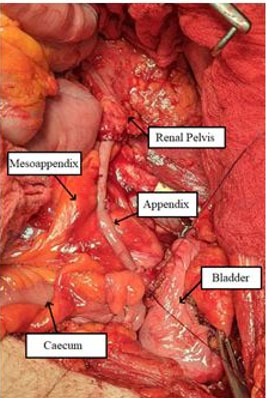
The bladder and the cecum were mobilized, the appendix was resected at the base to create a tube-like appearance, and was divided from the cecum with preservation of the mesoappendix. The appendix measured approximately 12 cm. Its distal part was anastomosed to the renal pelvis with separate stitches with 4/0 resorbable monofilament. Its proximal part was anastomosed to the bladder without creating an anti-reflux system, after placement of a transparietal mono J ureteral stent, also with separate stitches with 4/0 resorbable monofilament (Figure 1 and Figure 2).
On the digestive side, the patient developed colorectal anastomosis fistula, with bleeding on contact. The patient was treated with an endoscopic clip.
Urologically, the patient developed a urinoma at day 9 (D9) post-op, which resolved with continued ureteral and bladder catheter. The ureteral catheter was removed at D32 and the bladder catheter at D36 post-op.
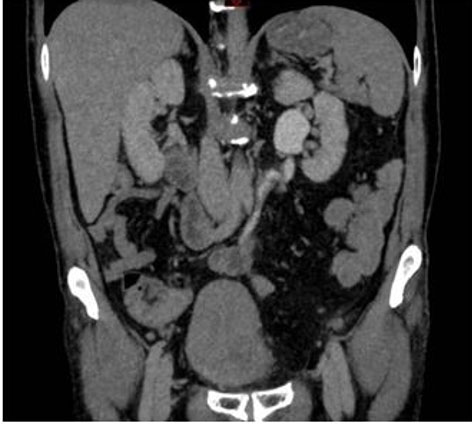
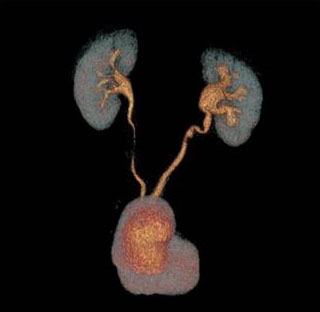
A follow-up computed tomography urography (CTU) was performed two months after the surgery, confirming the absence of urinary fistula and the good vascularization of the appendix (Figure 3 and Figure 4).
At the last follow-up in consultation, the patient had no backpain, and had not presented any urinary infection. The urinary creatinine was 70 µmol/mL. He had no metabolic problem either.

Discussion
Because of the large and proximal defect, the options for the patient were limited. We could have discussed left nephrectomy, cutaneous ureterostomy or Bricker diversion, transureteroureterostomy, digestive ureter replacement, and renal autotransplantation.
Nephrectomy was not an option for obvious reasons of preserving renal function. The patient had specified preoperatively that he was opposed to a cutaneous urinary diversion. The autotransplantation was not considered because of the small size of the remaining ureter and the external iliac vascular bypass. As the contralateral ureter was very thin, we decided not to perform transureteroureterostomy to avoid the risk of impacting the contralateral kidney. We proposed the ureter replacement using a digestive segment. Ileum ureteral replacement or Yang-Monti has been well studied in the literature and seems to be a reasonable option for long or very complex ureteral stricture with good long-term results [10],[11],[12],[13].
In the present clinical case the appendix was quite long and well vascularized. We preferred to perform an appendicular interposition to avoid a new digestive anastomosis and a more complex procedure. Its size permits to replace the complete ureter and to perform tension free anastomosis among the proximal left ureter and the bladder dome after mobilization of the cecum without the need for a Boari flap or psoic bladder. We decided to perform an antiperistaltic anastomosis for the appendix with the distal end to the proximal ureter in order to avoid any kind of traction and distortion of the mesoappendix. Studies in pediatric population have shown that both isoperistaltic or antiperistaltic were feasible [5],[6]. In some studies, the antiperistaltic position reduces the risks of ischemia secondary to a kinking of the appendicular meso [14],[15]. Nevertheless, the length of ureter did not permit to make a Lich Gregoir ureterovesical reimplantation, the antiperistaltic position of the appendix may therefore reduce the reflux to the kidney.
In order to protect the anastomosis, we placed a transparietal mono J ureteral stent, there is actually no recommendation for stenting or not in this case. Most of the cases were using double J stent for few weeks [5],[11],[16], even if tubeless appendicular interposition has already been published with good results [17].
Conclusion
In our experience, appendix interposition, when available and disease free, is a feasible and safe option for complete left ureteral defect in selected patients.
REFERENCES
1.
Hansen MH, Hayn M, Murray P. The use of bowel in urologic reconstructive surgery. Surg Clin North Am 2016;96(3):567–82. [CrossRef]
[Pubmed]

2.
Xiong S, Zhu W, Li X, Zhang P, Wang H, Li X. Intestinal interposition for complex ureteral reconstruction: A comprehensive review. Int J Urol 2020;27(5):377–86. [CrossRef]
[Pubmed]
3.
Ghoneim MA, Ali-El-Dein B. Replacing the ureter by an ileal tube, using the Yang-Monti procedure. BJU Int 2005;95(3):455–70. [CrossRef]
[Pubmed]
4.
Melnikoff AE. Sur le replacement de l’uretere par anse isolee de l’intestin grele. Rev Clin Urol 1912;1:601–3.
5.
Cao H, Zhou H, Yang F, et al. Laparoscopic appendiceal interposition pyeloplasty for long ureteric strictures in children. J Pediatr Urol 2018;14(6):551.e1–e5. [CrossRef]
[Pubmed]
6.
Dagash H, Sen S, Chacko J, et al. The appendix as ureteral substitute: A report of 10 cases. J Pediatr Urol 2008;4(1):14–9. [CrossRef]
[Pubmed]
7.
Obaidah A, Mane SB, Dhende NP, et al. Our experience of ureteral substitution in pediatric age group. Urology 2010;75(6):1476–80. [CrossRef]
[Pubmed]
8.
Burns ZR, Sawyer KN, Selph JP. Appendiceal interposition for ureteral stricture disease: Technique and surgical outcomes. Urology 2020;146:248–52. [CrossRef]
[Pubmed]
9.
Komyakov B, Ochelenko V, Guliev B, Shevnin M. Ureteral substitution with appendix. Int J Urol 2020;27(8):663–9. [CrossRef]
[Pubmed]
10.
Armatys SA, Mellon MJ, Beck SDW, Koch MO, Foster RS, Bihrle R. Use of ileum as ureteral replacement in urological reconstruction. J Urol 2009;181(1):177–81.
[Pubmed]
11.
Bilotta A, Wiegand LR, Heinsimer KR. Ureteral reconstruction for complex strictures: A review of the current literature. Int Urol Nephrol 2021;53(11):2211–9. [CrossRef]
[Pubmed]
12.
Ali-el-Dein B, Ghoneim MA. Bridging long ureteral defects using the Yang-Monti principle. J Urol 2003;169(3):1074–7. [CrossRef]
[Pubmed]
13.
Ali-El-Dein B, El-Hefnawy AS, D’ Elia G, et al. Long-term outcome of Yang-Monti ileal replacement of the ureter: A technique suitable for mild, moderate loss of kidney function and solitary kidney. Urology 2021;152:153–9. [CrossRef]
[Pubmed]
14.
Antonelli A, Zani D, Dotti P, Tralce L, Simeone C, Cunico SC. Use of the appendix as ureteral substitute in a patient with a single kidney affected by relapsing upper urinary tract carcinoma. ScientificWorldJournal 2005;5:276–9. [CrossRef]
[Pubmed]
15.
Dal Moro F, Terrosu G, Lorenzin D, et al. Complete substitution of the left ureter with vermicular appendix during hemicolectomy for cancer in an adult patient. Prog Urol 2020;30(10):547–9. [CrossRef]
[Pubmed]
16.
Jun MS, Stair S, Xu A, et al. A multi-institutional experience with robotic appendiceal ureteroplasty. Urology 2020;145:287–91. [CrossRef]
[Pubmed]
17.
Avci E, Atıcı SD, Uylas U, Kamer E. Stentless repair of left urethral defect with appendiceal interposition: A case report. Int J Surg Case Rep 2022;91:106805. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Marion Ghenassia - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jean Baptiste Bedel - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Louis Surlemont - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Christian Pfister - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lucie Vangheluwe - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Marion Ghenassia et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



