 |
Case Report
Superficial dorsal penile vein rupture mimicking penile fracture
1 Resident, Department of Urology, Dammam Medical Complex, Dammam, Saudi Arabia
2 Urology Consultant, Department of Urology, Dammam Medical Complex, Dammam, Saudi Arabia
3 Urology Specialist, Department of Urology, Dammam Medical Complex, Dammam, Saudi Arabia
Address correspondence to:
Ahmed Al Bazroon
Dammam,
Saudi Arabia
Message to Corresponding Author
Article ID: 100036Z15AB2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Al Bazroon A, Albassri A, Alabandi A, Alnemer M, Alhamwi H, Abu Alsaud S. Superficial dorsal penile vein rupture mimicking penile fracture. J Case Rep Images Urol 2023;8(2):14–17.ABSTRACT
Introduction: Superficial dorsal penile vein rupture is a rare penile emergency that mimics penile fracture. Many times, diagnosis will be uncertain as they both have similar symptoms and signs. Delay in treatment of penile fracture can lead to long-term sequelae like erectile dysfunction and thus prompt diagnosis and treatment are required.
Case Report: We report a case of a 35-year-old male patient with acute penile swelling and ecchymosis which developed during sexual intercourse suggesting penile fracture. Surgical exploration revealed rupture of superficial dorsal penile vein and no corporal injury. Hematoma was evacuated and vein was ligated. The patient had a good prognosis and reported maintained erectile function.
Conclusion: Superficial dorsal penile vein rupture is a rare penile emergency which usually has similar clinical features of penile fracture and hence called false penile fracture. If diagnosis is uncertain, surgical exploration is recommended for definitive diagnosis and to prevent potential long-term sequelae of untreated penile fracture.
Keywords: Coital injury, Penile fracture, Penile trauma, Superficial dorsal vein rupture
Introduction
Superficial dorsal penile vein rupture is a rare penile emergency that mimics penile fracture. Superficial dorsal penile vein rupture and penile fracture have similar clinical presentation as they both may present with acute penile swelling, ecchymosis, and pain that occurs during intercourse. In contrary, superficial dorsal penile vein fracture does not present with a click or snap sound which is frequently present with penile fracture. Also, no history of rapid detumescence in case of superficial dorsal vein rupture while it is present in cases of penile fracture. Diagnosis is usually by exclusion of penile fracture which is usually achieved by surgical exploration.
Case Report
A 35-year-old male patient who was medically free, presented to the emergency room complaining of penile swelling, ecchymosis, and pain that acutely occurred during intercourse. He reported vigorous intercourse, the use of local anesthetic and selective serotonin reuptake inhibitor (SSRI) pills to prolong erection and delay ejaculation. The patient was unsure if there is history of rapid detumescence, click, or snap sound as he was so worried and occupied by thinking about the swelling. He was able to void and had no history of lower urinary tract symptoms or hematuria. On examination, he was found to have penile swelling and ecchymosis limited to the penile shaft with normal appearance of glans (Figure 1). Laboratory investigations including complete blood count (CBC) and coagulation profile were within normal limits. No imagining study was performed to the patient.
Magnetic resonance imaging (MRI) was unavailable at our center at night time. We offered him the option of conservative treatment with plan to do MRI on the next day to rule out penile fracture. We also gave the other option which is surgical exploration to rule out penile fracture. After explaining the risks and complication of possibly undiscovered penile fracture, the patient elected to go for surgical exploration and did not want to wait for MRI.
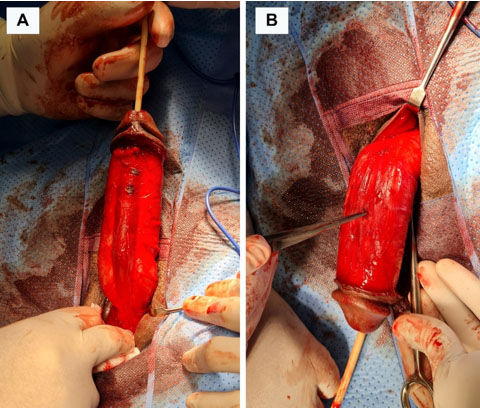
Penile exploration was done under general anesthesia via circumferential subcoronal incision and degloving of penile skin. Degloving was performed to the level of penile base and corporal bodies were exposed completely (Figure 2A). There was subcutaneous hematoma which spontaneously drained upon degloving and we had noted complete avulsion of superficial dorsal penile vein which was short, thrombosed, and there was no active bleeding at the time of exploration (Figure 2B). The vein was ligated. The patient had spontaneous erection during exploration, tunica albuginea was examined carefully and was intact (Figure 2A).

Discussion
Penile trauma is a rare medical emergency given the mobile nature of genitalia and its hidden anatomical position which contribute as protective factors from injuries. The most common penile emergency is penile fracture. Penile vascular injury is a rare condition, it mimics penile fracture and there are only few studies about it, mostly individual case reports.
The highest number of cases of superficial dorsal penile vein injury recorded by one group is 11 and was recorded by Kurkar and his colleagues [1]. The second highest number was recorded by Bar-Yosef and his colleagues [2]. In their study, 9 patients out of 18 patients with suspected penile fracture were found to have superficial dorsal penile vein injury [2].
Superficial dorsal penile vein tear clinically mimics penile fracture and in most of cases definitive diagnosis will be after surgical exploration. They both usually present after history trauma related to sudden change of position during vigorous sexual intercourse or manipulation of erected penis during masturbation. Patient with penile fracture usually presents with history of penile pain after hearing click sound, followed by rapid detumescence and penile swelling (eggplant deformity). However, click sound and rapid detumescence may not be present in case of superficial dorsal penile vein injury [1],[3],[4]. This was unclear in our patient as he could not recognize if he had any history of click sound or rapid detumescence.
Some authors have suggested circumcision as a risk factor for superficial dorsal penile vein injury as skin is tight in circumcised patient and will be stretched during erection which put veins at risk of being ruptured [1],[2],[4]. Other risk factors include vigorous sex and use of phosphodiesterase-5 (PDE-5) inhibitors [1]. In our case, the patient was circumcised, had history of vigorous sex and use of local anesthetics and SSRI to prolong erection and delay ejaculation.
Imaging may help in differentiation between true penile fracture and superficial dorsal penile vein injury. Ultrasound (US) can help by visualization of absence or presence tear in tunica albuginea or presence of hematoma beneath the skin. However, absence of tear does not exclude true penile fracture as the study is operator dependent and may miss tear in tunica albuginea [5]. Magnetic resonance imaging is the best modality of imaging to asses soft tissue and visualize possible tear in tunica albuginea but it is expensive and unavailable in many circumstances which limit its use [5]. Therefore, definitive diagnosis is usually by exclusion of penile fracture by surgical exploration.
Treatment of superficial dorsal penile vein injury can be by conservative or surgical management. Conservative management includes anti-inflammatory drugs and compressive dressing [4]. Even though it may resolve with conservative treatment, Kurkar and his colleagues recommended surgical exploration for any patient with suspected penile fracture [1]. This is recommended not only for definitive diagnosis but also to decrease the risk of significant sequalae and complications of penile fracture if missed or not treated surgically. Surgical management showed significant decrease risk of erectile dysfunction and penile deviation when compared to conservative treatment of penile fracture.
The prognosis of superficial dorsal penile vein injury is excellent if surgically treated. Surgical exploration permits to limit further bleeding by ligation of vein and thus preventing further expansion of hematoma and swelling. It also allows evacuation of hematoma and recovery will be faster (Figure 3). Our patient has excellent prognosis, rapid recovery, and maintained his erectile function.

Conclusion
Superficial dorsal penile vein rupture is rare penile emergency which usually have similar clinical features of penile fracture and hence called false penile fracture. Clinically, superficial dorsal penile vein rupture usually lacks the presence of click “snap” sound and rapid detumescence which usually present in penile fracture. Ultrasound and MRI may help in identifying presence or absence of defect in tunica albuginea. Magnetic resonance imaging is the best modality of imaging to asses soft tissue and visualize possible tear in tunica albuginea but it is expensive and unavailable in many circumstances which limit its use. In the absence of clinical features of penile fracture and absence of tunica albuginea tear, a case can be managed conservatively with satisfactory result. Surgical exploration is recommended for definitive diagnosis if uncertain. It allows identification of presence or absence of tunica albuginea tear, evacuation of hematoma, and ligation of any ruptured vein. It also decreases the risk of erectile dysfunction in case of penile fracture. Surgical treatment has good prognosis, rapid recovery, and maintained erectile function.
REFERENCES
1.
Kurkar A, Elderwy AA, Orabi H. False fracture of the penis: Different pathology but similar clinical presentation and management. Urol Ann 2014;6(1):23–6. [CrossRef]
[Pubmed]

2.
Bar-Yosef Y, Greenstein A, Beri A, Lidawi G, Matzkin H, Chen J. Dorsal vein injuries observed during penile exploration for suspected penile fracture. J Sex Med 2007;4(4 Pt 2):1142–6. [CrossRef]
[Pubmed]
3.
Feki W, Derouiche A, Belhaj K, et al. False penile fracture: Report of 16 cases. Int J Impot Res 2007;19(5):471–3. [CrossRef]
[Pubmed]
4.
Baran C, Topsakal M, Kavukcu E, Karadeniz T. Superficial dorsal vein rupture imitating penile fracture. Korean J Urol 2011;52(4):293–4. [CrossRef]
[Pubmed]
5.
El-Assmy A, El-Tholoth HS, Abou-El-Ghar ME, Mohsen T, Ibrahiem el HI. False penile fracture: Value of different diagnostic approaches and long-term outcome of conservative and surgical management. Urology 2010;75(6):1353–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ahmed Al Bazroon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ahmed Albassri - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ali Alabandi - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Murtadah Alnemer - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hazem Alhamwi - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shadi Abu Alsaud - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Ahmed Al Bazroon et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



