|
Case Report
Complex penile fracture after straddle injury: A case report
1 Urology Department, King Fahad Hospital, Hofuf, Saudi Arabia
Address correspondence to:
Ahmed Mousa Almuhanna
Urology Department, King Fahad Hospital, Hofuf,
Saudi Arabia
Message to Corresponding Author
Article ID: 100028Z15AA2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Almuhanna AM, Alessawi TH, Alghorairy B, Elkordy HM, Allali AM, Albagshi SS. Complex penile fracture after straddle injury: A case report. J Case Rep Images Urol 2023;8(1):1–4.ABSTRACT
Introduction: Penile fracture due to staddle injury is an underreported surgical emergency. Fall down in perinium can present with not only scrotum/perinium hematoma but can associated with more complicated injuries such as pelvis fracture, complex penile fracture with urethral injury, corpus cavernosal and spogiosium raptures. These findings lead to worse morbidity in the patient, especially in terms of sexual life and urinary symptoms. If such severe injuries are not properly managed, erectile dysfunction and urethral stricture can happen, leading to more complicated problems.
Case Report: A 23-year-old male presented to the emergency department with complaints of scrotal swelling and pain for three hours due to fall from height on perinium. He had classic signs of a urethral injury and penile fracture.
Conclusion: Penile fracture is not always spared injury and does not always occur during erection, but is sometimes associated with other injuries and in flaccid phase.
Keywords: Erectile dysfunction, Penile fracture, Penile injuries, Staddle injury, Trauma
Introduction
Penile fracture is an uncommon surgical emergency that occurs as a result of trauma to the erect penis mainly during intercourse [1]. The incidence of penile injuries is not reported because many patients do not seek medical care [2]. Penile fracture is a rupture of the tunica albuginea and most often occurs during sexual intercourse, usually after slipping the penis out from vagina and hitting the symphysis pubis [3].
Often patients present with a cracking or popping sound accompanied by immediate detumescence, followed by rapid swelling, ecchymosis, sharp pain, and deformity [4].
Penile fracture can be diagnosed after history taking, physical examination, and imaging. Prompt diagnosis and early surgical repair are essential to ensure a successful outcome and preserve erection [5].
It is uncommon for a penile fracture to occur during flaccid penis and associated with crural fracture, urethral injury, and spongiosa rupture. We report a rare case of a complicated penile fracture due to straddle injury from falling from height. It is uncommon for a penile fracture to occur during flaccid penis and associated with crural fracture, urethral injury, and spongiosa rupture. We report a rare case of a complicated penile fracture due to straddle injury from falling from height.
Case Report
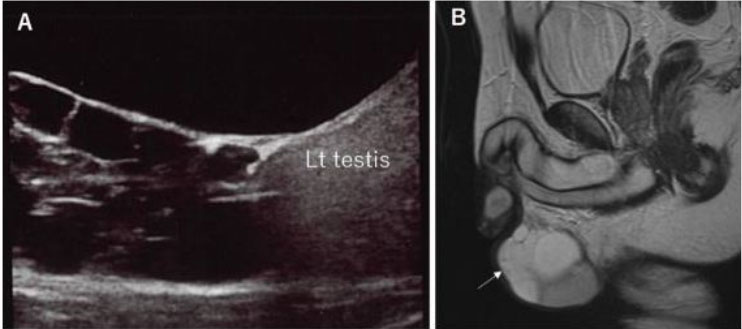
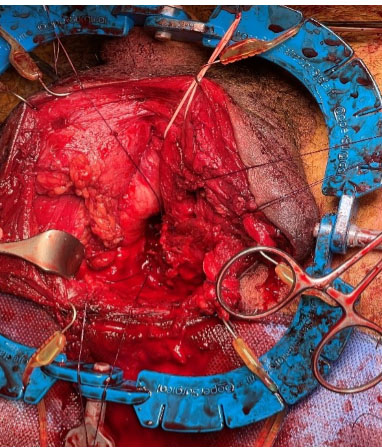
A 23-year-old male presented to the emergency department with complaints of scrotal swelling and pain for three hours due to fall from height on perinium. He had classic signs of a urethral injury and penile fracture. On physical examination he had blood at the meatus, scrotum swelling, butterfly perineal ecchymosis, and he was unable to void (Figure 1). Lab results were within normal values and radiological images done with X-ray confirmed a pelvis fracture (Figure 2), computed tomography (CT) showed right proximal corpora cavernosa and spongiosa ruptures (Figure 3) also there are no other associated organs injuries such as bowel, renal, ureters, and bladder injuries. Foley catheter was succeeded after gentle single attempt, he underwent scrotal exploration for hematoma evacuation (Figure 4) and right proximal corpora cavernosa and spongiosa repair (Figure 5 and Figure 6). During hospital course post-procedure daily dressing, antibiotics, and Foley kept for three weeks then periurethral retrograde urethrogram (RUG) was done outside our hospital without any extravasation. Currently the patient voids freely.





Discussion
Penile fracture is an underreported emergent urological condition. It is underreported because many patients do not seek medical attention due to embarrassment, shame, or lack of guidance [2]. There are many activities that can result in penile fracture such as severely bending the penis during erection either in sexual intercourse or during self-manipulation to achieve detumescence [3]. The increased risk of penile fractures during tumescence is related to the tunica albuginea stretching forcefully.
There is an extensive review made by Eke for 183 publications on 1331 cases. The median age of patients were 35 years. Clinical picture of penile fracture included sudden penile pain, detumescence, voiding difficulties, penile swelling, and deviation. In addition, other such injuries that are associated with penile fracture are urethral rupture, complications of penile fracture, penile plaque, and erectile dysfunction [1].
The management of penile fracture is surgical repair. However, recent studies have revealed that long-term outcomes of early versus delayed repair in patients without urethral involvement are similar [6],[7]. In our case, surgical repair was offered early in the course of the presentation as the patient has complicated penile fracture associated with urethral injury and scrotal hematoma. Hematoma was evacuated, corpora cavernosa and spongiosa were repaired and Foley catheter was inserted. Recently once such case was published, where a 36-year-old male sustained a staddle injury presented with butterfly ecchymosis, urethral injury, and corpora cavernosa injury but the attempt to insert the Foley catheter was failed. Retrograde urethrogram was done and showed a bulbar urethral injury. The patient underwent a surgical exploration and repair and suprapubic catheter insertion [8]. Our case was referred to another private hospital for follow-up and the patient voids freely with good erection.
Conclusion
Penile fracture is not always a spared injury and does not occur during erection but sometimes it is associated with other injuries and in flaccid phase. In this case, CT imaging was useful in delineating the location and side of the proximal corpora cavernosa and spongiosa injuries and informed surgical planning. Long-term outcomes following surgical correction of proximal corpora injuries are not clear because of infrequency of this type of penial fracture.
REFERENCES
1.
Eke N. Fracture of the penis. Br J Surg 2002;89(5):555– 65. [CrossRef]
[Pubmed]

2.
Krishna Reddy SV, Shaik AB, Sreenivas K. Penile injuries: A 10-year experience. Can Urol Assoc J 2014;8(9–10):E626–31. [CrossRef]
[Pubmed]
3.
Kachewar S, Kulkarni D. Ultrasound evaluation of penile fractures. Biomed Imaging Interv J 2011;7(4):e27. [CrossRef]
[Pubmed]
4.
Kozacioglu Z, Degirmenci T, Arslan M, Yuksel MB, Gunlusoy B, Minareci S. Long-term significance of the number of hours until surgical repair of penile fractures. Urol Int 2011;87(1):75–9. [CrossRef]
[Pubmed]
5.
Nasser TA, Mostafa T. Delayed surgical repair of penile fracture under local anesthesia. J Sex Med 2008;5(10):2464–9. [CrossRef]
[Pubmed]
6.
Boncher NA, Vricella GJ, Jankowski JT, Ponsky LE, Cherullo EE. Penile fracture with associated urethral rupture. Case Rep Med 2010;2010:791948. [CrossRef]
[Pubmed]
7.
Naraynsingh V, Hariharan S, Goetz L, Dan D. Late delayed repair of fractured penis. J Androl 2010;31(2):231–3. [CrossRef]
[Pubmed]
8.
William JM, Anderson JB, Laborde EL. Penile fracture caused by straddle injury to a nonerect penis. Urology 2020;142:e47–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ahmed Mousa Almuhanna - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Turki H Alessawi - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Basim Alghorairy - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hany M Elkordy - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ali M Alali - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sara Sameer Albagshi - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Ahmed Mousa Almuhanna et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.