|
Case Report
Right inguinal hernia containing ureter: A rare “tortuous” surprise for general surgeons and urologists
1 Urology Department, Sirai Hospital, Carbonia, Italy
2 Chief of Urology Department, ARNAS G. Brotzu, Cagliari and Former Chief of Urology Department, Sirai Hospital, Carbonia, Italy
Address correspondence to:
Riccardo Farci
Urology Department, Sirai Hospital, Via dell’Ospedale, 09013 Carbonia,
Italy
Message to Corresponding Author
Article ID: 100052Z15RF2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Farci R, Solinas A. Right inguinal hernia containing ureter: A rare “tortuous” surprise for general surgeons and urologists. J Case Rep Images Urol 2025;10(1):13–16.ABSTRACT
Inguinal hernia is a very common pathology worldwide. Global incidence is about 4–5%. The most commonly involved organs are the abdominal viscera. As far as urology is concerned, urinary bladder is involved in approximately 0.5–4% of all inguinal hernias, while finding the ureters is truly a rarity, about 150 cases worldwide. Ureteral hernias could be an incidental finding but it is important to know about their existence to avoid injury during surgery. We present the case of a 71-year-old man with a finding of right ureteral hernia incidentally diagnosed during computed tomography (CT) scan for an abdominal abscess.
Keywords: Hernia containing ureter, Inguinal hernia, Renal ptosis, Ureteral hernia
Introduction
Inguinal hernia is a very common pathology worldwide. Global incidence is about 4–5%, with men involved 8 times more than women, specially over 50 years old ones, bilateral in 15–20% of cases.
It is therefore intuitive that inguinal hernia repair is one of the most performed surgical procedures worldwide [1]. The most commonly involved organs are the abdominal viscera. As far as urology is concerned, the urinary bladder is involved in approximately 0.5–4% of all inguinal hernias, while finding the ureters is truly a rarity, about 150 cases worldwide [2].
They can both be identified during inguinal hernia surgery or during CT scan performed for other reasons [3], it is crucial to be aware of the existence of such kind of anatomic variations to avoid injuries to the ureters.
They can both be identified during inguinal hernia surgery or during CT scan performed for other reasons [3], it is crucial to be aware of the existence of such kind of anatomic variations to avoid injuries to the ureters.
Ureteral hernias are usually indirect and can be distinguished in two types [4]:
- paraperitoneal ones, representing 80% of case, usually accompanied by herniation of other abdominal viscera because of the presence of adherence of the peritoneum or peritoneal sac with the ureter;
- extraperitoneal, they can contain ureter alone or in combination with retroperitoneal fat, they lack the peritoneal sac, they are irreducible and usually congenital and can be associated with other anatomical anomalies such as renal ptosis or double district.
Ureteral hernias may be asymptomatic or may present with flank pain secondary to obstructive uropathy, recurrent pyelonephritis, urosepsis, and hematuria.
Case Report
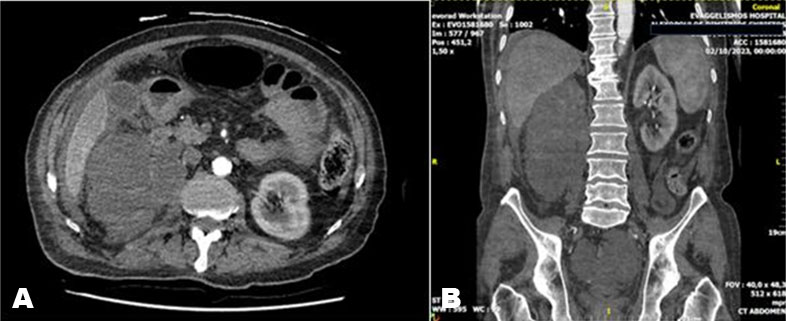
CB, a 71-year-old man with atrial fibrillation, type 2 diabetes mellitus, obesity, and arterial hypertension presented to the Emergency Department with a history of acute, diffuse abdominal pain associated with fever up to 39°C. Blood tests show the presence of a marked neutrophilic leukocytosis, increased inflammation indices, and normal creatinine values. Physical examination revealed an acute abdomen and a large, right inguinoscrotal hernia, which the patient said was inveterate. For this reason, after specialistic consultation, he was admitted to the General Surgery Department and underwent a complete abdominal contrast-enhanced CT scan, which revealed a large multi-chambered abscess collection starting from the cecum, on which there are numerous ileal loops adhered to each other and distended in relation to intestinal obstruction, highly suspicious for complicated acute appendicitis. The presence of the right ureteral hernia is instead an incidental finding. The ureter is described as prolapsed inside the hernial sac, with a tortuous course, not entirely assessable, accompanied by retroperitoneal fat and right renal ptosis, with the lower pole of the kidney in proximity to the hernial portal (Figure 1). However, hydronephrosis was not detected.
Due to the patient’s severe clinical conditions, after a collegial consultation between general surgeons and urologists, it was decided to perform a retrograde pyelography and positioning of a 6 Ch monoJ ureteral catheter as a landmark for the laparotomy procedure, postponing the correction of the ureteral hernia to a later time.
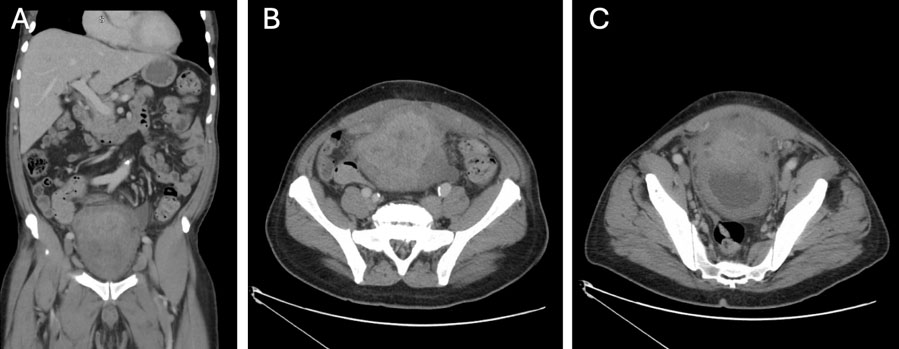
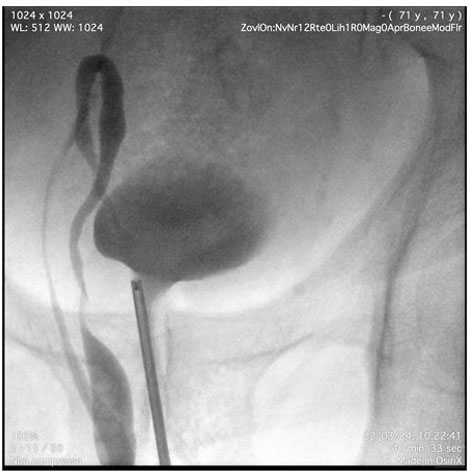
Pyelography was performed using an 8 Ch ureteroscope. After inserting the instrument into the bladder, the right ureteral meatus was identified and pyelography was performed with an open-ended catheter. The tortuosity of the ureter was confirmed, describing a double loop into the scrotum (Figure 2 and Figure 3). After identifying the renal pelvis, approximately in the right iliac fossa, a 6 Ch monoJ ureteral catheter was positioned.
The acute abdomen was instead caused by gangrenous appendicitis, so General Surgeons proceeded to appendectomy, viscerolysis, and drainage of the abscess. No problem was encountered regarding the ureter. After the surgical procedure the monoJ ureteral catheter was removed and the patient did not have any symptoms related to ureteral hernia, but was discharged about 25 days after surgery because of bilateral pneumonia and acute heart failure that needed intensive care.


Discussion
Ureteral hernias are an uncommon condition, about 150 cases described worldwide [2], specially in patients with native kidneys, while they are more common in patients with transplanted ones [5]. They can be paraperitoneal, about 80% of cases due to adherence between the ureter with peritoneum or extraperitoneal, containing the ureter and retroperitoneal fat, usually congenital and associated with other abnormalities such renal ptosis.
Clinical manifestations vary from asymptomatic to acute renal failure or urosepsis, but they can also cause hematuria, nocturia, suprapubic pain or pressure, dysuria, and urgency. Frequently diagnosed during or post-inguinal hernia surgery repair, they can represent a trap for general surgeons [6], while they rarely diagnosed pre-operatively, usually in CT scan taken for other reasons [7]. Routine imaging to identify ureteral hernias is unlikely to be cost-effective.
In this case we suspect a retroperitoneal form since it is inveterate, big right-sided, accompanied by renal ptosis on CT scan. Moreover during the appendectomy and drainage of the abscess no peritoneal sac was found engaging the inguinal canal, but ultimately definitive diagnosis between paraperitoneal versus extraperitoneal hernias is an intraoperative finding [2].
Trying to solve the diagnostic lack of this rare ureteral pathology we think it may be reasonable to propose a 3D contrast-enhanced CT scan, as previously proposed by Pareja-López et al. [8], for all patients with risk factors like male sex, obesity, and big right-sided hernias [9].
In these cases the diagnostics can dramatically change surgical approaches and consequentially surgical outcomes, as it can avoid creating iatrogenic damage to the ureters.
Beyond all these reasons, the absolute certainty of a ureteral hernia is obtained with a retrograde pyelography.
In case obstructive uropathy retrograde pyelography also consents ureteric stent placement, usually a long monoJ type is required because of tortuosity and length of ureters, but sometimes it is necessary the placement of nephrostomic tube.
Although this patient had no signs of obstructive uropathy, we decided to perform retrograde pyelography and monoJ ureteric placement to precisely be conscious of right ureter anatomy and to provide General Surgeons a precious landmark, avoiding iatrogenic traumas.
As mentioned above, the correction of ureteral hernias depends on the clinical findings, and can vary from urgent urinary diversion in case of urosepsis or obstructive uropathy, to elective correction.
We think that the decision of elective correction must be taken in a multidisciplinary approach between Urologists and General Surgeons, since specific techniques of one or the other discipline may be necessary depending on the case.
Without going into the merits of the surgical techniques for correcting inguinal hernias, the Urologist can be involved in case it is necessary to perform resection and reanastomosis of the ureter or more complex techniques of ureteral reimplantation [10].
In this specific case we decided to propose a conservative approach due to the patient’s critical condition, postponing surgical correction as soon as the patient’s condition allows it.
Conclusion
Ureteral hernias are an extremely rare disease, usually they are incidental findings during hernia repair surgery or during CT scan performed for other reasons. As they can be a trap for both urologists and general surgeons, it is important to be aware about their existence to ensure the best possible treatment for the patient. From the literature we learned that there are two types of ureteral hernias and that there are some risk factors, such as male sex, obesity, and right-sidedness. In these cases it may be feasible, also from a cost–benefit perspective, to undergo the patient to a contrast-enhanced 3D CT scan and possibly to a retrograde pyelography to avoid iatrogenic trauma to the ureter and improve outcomes. We also understood that a multidisciplinary approach is essential for the treatment of ureteral hernias since specific surgical techniques of both general surgery and urology may be necessary.
REFERENCES
1.
Bay-Nielsen M, Kehlet H, Strand L, et al. Quality assessment of 26,304 herniorrhaphies in Denmark: A prospective nationwide study. Lancet 2001;358(9288):1124–8. [CrossRef]
[Pubmed]

2.
Pucheril D, Chun B, Dalela D, Abdollah F, Laker SA, Rogers CG. Robot-assisted laparoscopic repair of extraperitoneal ureteral inguinal hernia with mesh placement. J Endourol Case Rep 2017;3(1):97–100. [CrossRef]
[Pubmed]
3.
Bertolaccini L, Giacomelli G, Bozzo RE, Gastaldi L, Moroni M. Inguino-scrotal hernia of a double district ureter: Case report and literature review. Hernia 2005;9(3):291–3. [CrossRef]
[Pubmed]
4.
Beebe K, Muhonen J, Giuseppucci P, Esper C. A rare case of an inguinal hernia-containing (extraperitoneal) ureter. Am J Case Rep 2021;22:e930911. [CrossRef]
[Pubmed]
5.
Osman Y, Ali-El-Dein B, El-Leithy R, Shokeir A. Sliding hernia containing the ureter—A rare cause of graft hydroureteronephrosis: A case report. Transplant Proc 2004;36(5):1402–4. [CrossRef]
[Pubmed]
6.
Yahya Z, Al-Habbal Y, Hassen S. Ureteral inguinal hernia: An uncommon trap for general surgeons. BMJ Case Rep 2017;2017:bcr2017219288. [CrossRef]
[Pubmed]
7.
van den Berg JC, de Valois JC, Go PM, Rosenbusch G. Detection of groin hernia with physical examination, ultrasound, and MRI compared with laparoscopic findings. Invest Radiol 1999;34(12):739–43. [CrossRef]
[Pubmed]
8.
Pareja-López Á, Sevilla-Cecilia C, Pey-Camps A, Dominguez-Tristancho JL, Muteb M. Ureteroinguinal hernia. Cir Esp 2015;93(8):e89–90. [CrossRef]
[Pubmed]
9.
Laurie BD. Unexpected ureter within an inguinal hernia. Cureus 2023;15(3):e36691. [CrossRef]
[Pubmed]
10.
McKay JP, Organ M, Bagnell S, Gallant C, French C. Inguinoscrotal hernias involving urologic organs: A case series. Can Urol Assoc J 2014;8(5–6):E429–32. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Riccardo Farci - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andrea Solinas - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Riccardo Farci et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.