 |
Case Report
Management of forgotten complex ureteral stent with complete incrustation
1 Resident 5 year, Urology Department, University Hospital Center Hassan II of Fez, Fez, Morocco
2 Professor, Urology Department, University Hospital Center Hassan II of Fez, Fez, Morocco
3 Head of the Department, Urology Department, University Hospital Center Hassan II of Fez, Fez, Morocco
Address correspondence to:
Mohamed Amine Malki
737 LOT Almansour, Meknes,
Morocco
Message to Corresponding Author
Article ID: 100035Z15MM2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Malki MA, Ahsaini M, Mellas S, Tazi MF, El Ammari J, El Fassi J, Farih MH. Management of forgotten complex ureteral stent with complete incrustation. J Case Rep Images Urol 2023;8(2):9–13.ABSTRACT
This case report describes the therapeutic management of a 23-year-old patient with encrusted double J stent in the bladder. A mini-cystotomy was performed to extract the encrusted lower end of the stent, followed by the placement of a new stent. Subsequently, flexible ureteroscopy with laser lithotripsy was conducted to remove renal calculi. The postoperative outcomes were favorable, with pain regression and absence of residual stones. A multidisciplinary and individualized approach is crucial in the management of encrusted double J stents to optimize clinical outcomes and prevent long-term complication.
Keywords: Double J stent, Incrustation, Stones
Introduction
Urolithiasis, the formation of urinary tract stones, is a common condition affecting a significant proportion of the population worldwide. Double J stents are often used in the management of urolithiasis [1], but they can become encrusted, leading to various complications [2],[3]. This article presents a case report of a 23-year-old patient with encrusted double J stent and discusses the clinical presentation, diagnostic evaluation, therapeutic interventions, and postoperative outcomes.
Understanding the challenges and effective management strategies for encrusted double J stents is crucial for improving patient outcomes [3],[4],[5].
Case Report
We present a case report of a 23-year-old patient who had been followed for urolithiasis for the past four years. The patient initially received a left ureteral stent placement for obstructive pyelonephritis and was scheduled for ureterorenoscopy (URS) with laser lithotripsy. However, the patient was lost to follow-up. Currently, the patient presents with lower back pain and irritative symptoms, including frequent urination and burning sensation during urination.
Upon clinical examination, the patient was stable hemodynamically and respiratorily, with a heart rate of 73 bpm, blood pressure of 13/7 mmHg, and afebrile at 36.8°C. Flank tenderness was noted on the left side, but there was no costovertebral angle tenderness. The rest of the examination was unremarkable.
The laboratory investigations revealed hemoglobin levels of 13.8 g/dL, a white blood cell count of 13,000/µL, C-reactive protein levels of 45 mg/L, urea levels of 0.23 g/L, and creatinine levels of 7 mg/L. Urine culture and sensitivity testing showed Escherichia coli sensitive to third-generation cephalosporins.
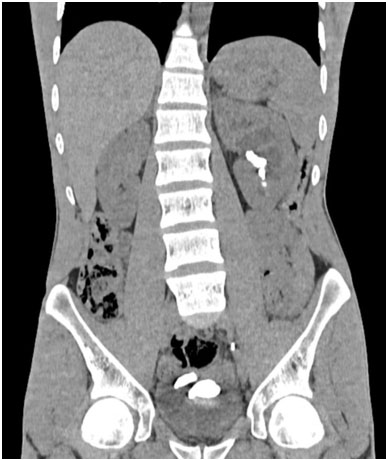
A computed tomography scan performed on February 8, 2023 revealed a left renal stone measuring 20×8 mm in the renal pelvis, with calcific density causing significant upstream dilation and stasis stones involving various calyceal groups. The double J stent was in place, with the upper loop positioned at the level of the iliac ureter, and signs of encrustation were observed at the lower loop (Figure 1 and Figure 2).
Therapeutic management
Our patient initially underwent mini-cystotomy for the extraction of the encrusted lower end of the stent and subsequent placement of a new double J stent. Subsequently, the patient was scheduled for flexible ureteroscopy with laser lithotripsy for the extraction of renal calculi.
Postoperative outcomes
The postoperative course was uneventful, with a significant reduction in pain. The patient is currently considered “stone free,” indicating the successful removal of the renal calculi (Figure 3).


Discussion
Encrustation of double J stents poses a significant challenge in the management of urolithiasis [3],[4]. It can lead to various complications, including recurrent urinary tract infections, obstruction, and renal damage. Therefore, prompt and appropriate therapeutic interventions are necessary to address this complication.
The use of a mini-cystotomy allowed for the extraction of the encrusted lower end of the stent, which was crucial in resolving the patient’s symptoms and preventing further complications [2]. The placement of a new double J stent ensured the restoration of urinary tract patency and facilitated subsequent procedures, such as flexible ureteroscopy [6].
Flexible ureteroscopy with laser lithotripsy is a minimally invasive approach for the management of renal calculi [6]. It offers the advantage of precise stone fragmentation and retrieval while minimizing the need for open surgery. In this case, it provided an effective method for removing the renal calculi and achieving a “stone-free” status.
The successful outcomes observed in this case highlight the importance of a multidisciplinary approach in the management of encrusted double J stents and associated renal calculi [3],[4]. Close collaboration between urologists, interventional radiologists, and nephrologists allowed for the timely and appropriate selection of therapeutic interventions tailored to the patient’s specific needs.
However, it is important to note that each case of encrusted double J stents is unique [4],[7],[8], and management strategies should be individualized based on factors such as the extent of encrustation, patient comorbidities, and available resources. Long-term follow-up and preventive measures, such as regular surveillance and stent cleaning protocols, are crucial to minimize the risk of future complications and ensure optimal patient outcomes [3].
Conclusion
This case highlights the successful therapeutic management of encrusted double J stents through a combination of mini-cystotomy, stent replacement, and flexible ureteroscopy with laser lithotripsy. These interventions effectively addressed the patient’s symptoms, removed the encrusted stent segment, and achieved stone-free status. Further research and experience are needed to develop standardized protocols and guidelines for the management of encrusted double J stents, considering both short-term and long-term outcomes.
REFERENCES
1.
Ngo TC, Lee JJ, Gonzalgo ML. Ureteral stenting after ureteroscopy for stone disease: A systematic review and meta-analysis. J Urol 2008;179(2):424–30.

2.
Tang J, Xu Z, Xie H, et al. Prevention and management of ureteral stent complications: A systematic review and meta-analysis. J Endourol 2018;32(9):794–809.
3.
Taha A, Al-Marhoon M, Jacob S, et al. Management of forgotten ureteral stents with or without encrustation. Urol Ann 2016;8(4):470–5.
4.
Chuang YC, Su YJ, Chiang PH, et al. Encrusted ureteral stents: Clinical experience and review of the literature. Urol Sci 2015;26(4):231–5.
5.
Cheung MC, Lee F, Leung YL, Wong BB, Tam PC. Encrusted double-J ureteral stent: Management options. Urology 2004;63(5):841–3.
6.
Salem HK. A prospective randomized study comparing shock wave lithotripsy and semirigid ureteroscopy for the management of proximal ureteral calculi. Urology 2009;74(6):1216–21. [CrossRef]
[Pubmed]
7.
Osman Y, El-Tabey N, Refaie HF, El-Hefnawy AS, Eraky I, Shabaan A. Encrusted ureteral stents: Evaluation and endourologic management. Urology 2001;58(4):526–32.
8.
Dangle PP, Viswaroop BS, Pillai BS, Desai MR. Management of retained ureteral stents with forgotten or displaced ends. J Endourol 2005;19(1):54–7.
SUPPORTING INFORMATION
Author Contributions
Mohamed Amine Malki - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mustapha Ahsaini - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Soufiane Mellas - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamed Fadl Tazi - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jalal El Ammari - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jamal El Fassi - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
My Hassan Farih - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Mohamed Amine Malki et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



