|
Case Report
The intravesical migration of a lost intrauterine device
1 Senior Doctor, Urology, Borromäus Hospital in Leer, Leer, Germany
2 Director, Department for Urology in Borromäus Hospital in Leer, Germany
Address correspondence to:
H Hatem
Senior Doctor, Urology, Borromäus Hospital in Leer, Leer,
Germany
Message to Corresponding Author
Article ID: 100011Z15HH2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Hatem H, Leifeld J. The intravesical migration of a lost intrauterine device. J Case Rep Images Urol 2020;5:100011Z15HH2020.ABSTRACT
The intravesical migration of intrauterine devices (IUDs) has rarely been reported. In many cases, diagnosis is missed or delayed. We present a case of a 34-year-old female patient with intravesical migration of an IUD, which was thought to be lost. To check for the presence of the IUD, which had dislodged, the patient’s gynecologist inserted another one. Later, the patient presented with recurrent urinary infections. A diagnosis was reached through cystoscopy; the migrated device was visible through the posterior wall. We removed the device transurethrally. This case is presented to highlight the importance of following up with patients with IUDs to avoid potential complications.
Keywords: Intrauterine device , Intravesical, Perforation
Introduction
Intrauterine devices (IUD) are generally considered a safe, reliable, and economical contraception method. One of their potential complications is intravesical migration, which can present as dysuria, recurrent infections, or dyspareunia.
If there is any suspicion of this condition, it can be investigated simply through ultrasound or plain film. The most common approach to removing an IUD is transurethral resection. If large stones are present, open or laparoscopic approaches are more appropriate. We report on the case of a patient with intravesical migration of an IUD that was thought to be lost.
Case Report
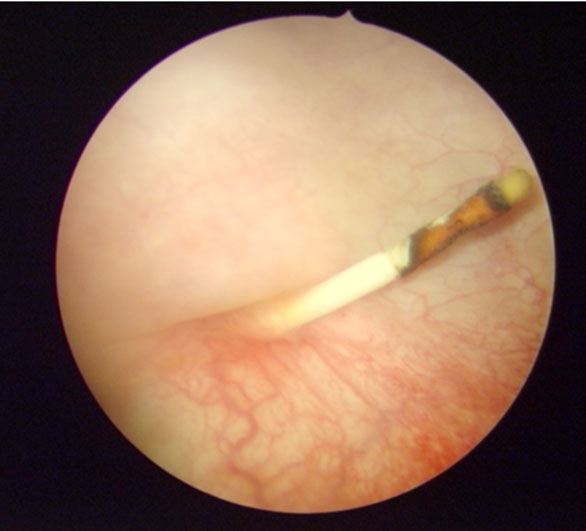
We report on a 34-year-old female patient who complained of recurrent cystitis for many years. To address this issue, the patient went to a urology outpatient clinic. As part of our study, a cystoscopy was performed, and the migrated IUD was seen through the posterior wall of the bladder. The IUD had first been inserted seven years earlier, and the patient noted that she had not noticed losing it. Four years after that, her gynecologist had inserted another one without investigating whether the first one was still intracorporeal. The patient was admitted to our clinic to remove the IUD.
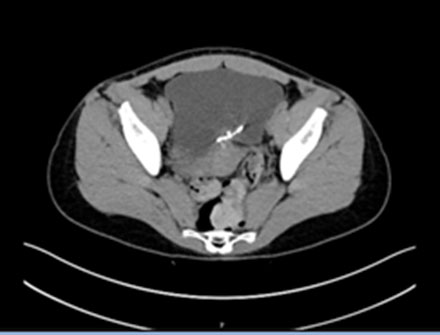
To determine a diagnosis, we performed an abdominal computed tomography (CT) scan to reveal the position of the migrated device and the status of her anatomical condition.
With the patient under general anesthesia, we removed the IUD, performing a superficial, transurethral resection of the bladder mucosa. The urinary catheter was removed seven days later, after a cystogram showed no evidence for a fistula or extravasation (Figure 1). The recurrent infections have since been entirely resolved.

Discussion
The IUD is the most widely used contraceptive worldwide due to its safety, activity, and affordability. However, despite its safety, some patients experience complications, including pelvic inflammatory disease (PID), uterine perforation, heavy bleeding, dysmenorrhea, and unplanned pregnancy [1].
Such migration is rare—in 0.003–0.87% [2] or in 1.9–3.6 per 1000 insertions [3]. A dislodged IUD could be located in different organs, such as the mentum, rectosigmoid, peritoneum, bladder, appendix, small bowel, adnexa, or even iliac vein. In about 200 cases of uterine perforation reviewed from 1991 to 2015, Kart and colleagues found 90 cases of intravesical migration [4].
Many factors can lead to the migration of the IUD, such as actions by inexperienced staff or a patient’s atypical anatomical issues, such as an extreme posterior uterine position [5],[6]. However, it seems that perforation occurs during or after insertion, or as a slow process that leads to migration, as in our case [2].
Sometimes this migration causes no complaints. In others, however, it is associated with complications, including dysuria, dyspareunia, or vesical calculus. In our case, the patient reported recurrent infections.
A migration diagnosis can be reached through ultrasound and plain film [7]. In our case, the diagnosis was confirmed through a cystoscopy performed by an outpatient urologist. To investigate further, we decided to perform a CT scan to ensure the extension and location of the IUD (Figure 2 and Figure 3).
Incomprehensibly, the patient’s gynecologist had not undergone any examination, such as an ultrasound or plain film, to check for the presence or position of the first IUD, which was believed to be lost.
With the patient under anesthesia, we performed a transurethral resection to remove the IUD (Figure 4). In standard treatment, a minimally invasive approach should be chosen [8]. A more invasive approach, such as a cystotomy, may be required if large stones are present or in the case of associated fistula formations [9].

Conclusion
Although the intravesical migration of an IUD is rare, it should be kept in mind, and every female patient complaining of recurrent infections should be interviewed regarding her IUD history.
REFERENCES
1.
Aggarwal S, Jindal RP, Deep A. Intravesical migration of intrauterine contraceptive devices with stone formation. J Family Med Prim Care 2014;3(4):449– 51. [CrossRef]
[Pubmed]

2.
Markovitch O, Klein Z, Gidoni Y, Holzinger M, Beyth Y. Extrauterine mislocated IUD: Is surgical removal mandatory? Contraception 2002;66(2):105–8. [CrossRef]
[Pubmed]
3.
Farmer M, Webb A. Intrauterine device insertion-related complications: Can they be predicted? J Fam Plann Reprod Health Care 2003;29(4):227–31. [CrossRef]
[Pubmed]
4.
Kart M, Gülecen T, Üstüner M, Çiftçi S, Yavuz U, Özkürkçügil C. Intravesical migration of missed intrauterine device associated with stone formation: A case report and review of the literature. Case Rep Urol 2015;2015:581697. [CrossRef]
[Pubmed]
5.
Dimitropoulos K, Skriapas K, Karvounis G, Tzortzis V. Intrauterine device migration to the urinary bladder causing sexual dysfunction: A case report. Hippokratia 2016;20(1):70–2.
[Pubmed]
6.
Vagholkar S, Vagholkar K. Secondary vesical calculus resulting from migration of an intrauterine contraceptive device. Case Rep Obstet Gynecol 2012;2012:603193. [CrossRef]
[Pubmed]
7.
El-Diasty TA, Shokeir AA, el-Gharib MS, Sherif LS, Shamaa MA. Bladder stone: A complication of intravesical migration of Lippes loop. Scand J Urol Nephrol 1993;27(2):279–80. [CrossRef]
[Pubmed]
8.
Guner B, Arikan O, Atis G, Canat L, Çaskurlu T. Intravesical migration of an intrauterine device. Urol J 2013;10(1):818–20.
[Pubmed]
9.
El-Hefnawy AS, El-Nahas AR, Osman Y, Bazeed MA. Urinary complications of migrated intrauterine contraceptive device. Int Urogynecol J Pelvic Floor Dysfunct 2008;19(2):241–5. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
H Hatem - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jörg Leifeld - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 H Hatem et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.